{"title":"Normal Appearing Ischaemic Brain Tissue on CT and Outcome After Intravenous Alteplase.","authors":"Grant Mair, Joanna M Wardlaw","doi":"10.3389/fradi.2022.902165","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>The visibility of ischaemic brain lesions on non-enhanced CT increases with time. Obviously hypoattenuating lesions likely represent infarction. Conversely, viable ischaemic brain lesions may be non-visible on CT. We tested whether patients with normal appearing ischaemic brain tissue (NAIBT) on their initial CT are identifiable, and if NAIBT yields better outcomes with alteplase.</p><p><strong>Methods: </strong>With data from the Third International Stroke Trial (IST-3, a large randomized-controlled trial of intravenous alteplase for ischaemic stroke) we used receiver-operating characteristic analysis to find a baseline National Institutes of Health Stroke Scale (NIHSS) threshold for identifying patients who developed medium-large ischaemic lesions within 48 h. From patients with baseline CT (acquired <6 h from stroke onset), we used this NIHSS threshold for selection and tested whether favorable outcome after alteplase (6-month Oxford Handicap Score 0-2) differed between patients with NAIBT vs. with those with visible lesions on baseline CT using binary logistic regression (controlled for age, NIHSS, time from stroke onset to CT).</p><p><strong>Results: </strong>From 2,961 patients (median age 81 years, median 2.6 h from stroke onset, 1,534 [51.8%] female, 1,484 [50.1%] allocated alteplase), NIHSS>11 best identified those with medium-large ischaemic lesions (area under curve = 0.79, sensitivity = 72.3%, specificity = 71.9%). In IST-3, 1,404/2,961 (47.4%) patients had baseline CT and NIHSS>11. Of these, 745/1,404 (53.1%) had visible baseline ischaemic lesions, 659/1,404 (46.9%) did not (NAIBT). Adjusted odds ratio for favorable outcome after alteplase was 1.54 (95% confidence interval, 1.01-2.36), p = 0.045 among patients with NAIBT vs. 1.61 (0.97-2.67), <i>p</i> = 0.066 for patients with visible lesions, with no evidence of an alteplase-NAIBT interaction (<i>p</i>-value = 0.895).</p><p><strong>Conclusions: </strong>Patients with ischaemic stroke and NIHSS >11 commonly develop sizeable ischaemic brain lesions by 48 h that may not be visible within 6 h of stroke onset. Invisible ischaemic lesions may indicate tissue viability. In IST-3, patients with this clinical-radiological mismatch allocated to alteplase achieved more favorable outcome than those allocated to control.</p>","PeriodicalId":73101,"journal":{"name":"Frontiers in radiology","volume":"2 ","pages":"902165"},"PeriodicalIF":2.3000,"publicationDate":"2022-06-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10364986/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fradi.2022.902165","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aims: The visibility of ischaemic brain lesions on non-enhanced CT increases with time. Obviously hypoattenuating lesions likely represent infarction. Conversely, viable ischaemic brain lesions may be non-visible on CT. We tested whether patients with normal appearing ischaemic brain tissue (NAIBT) on their initial CT are identifiable, and if NAIBT yields better outcomes with alteplase.
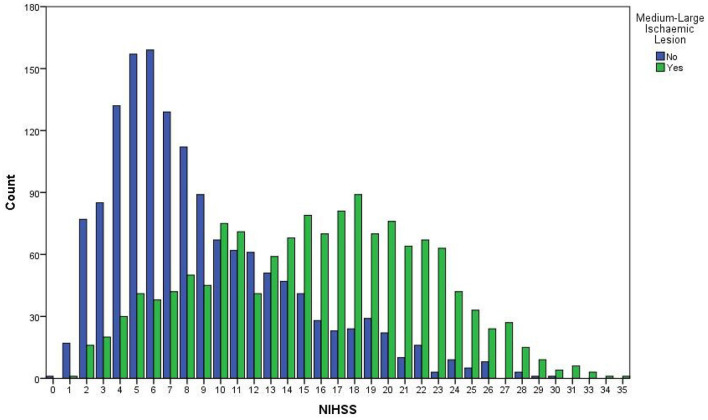
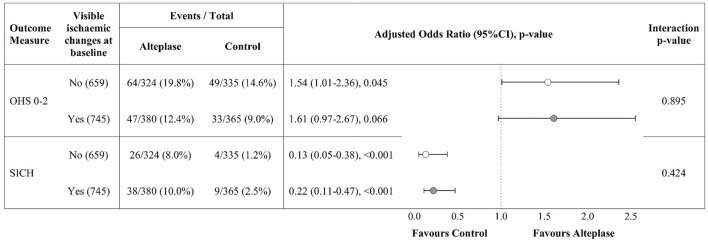
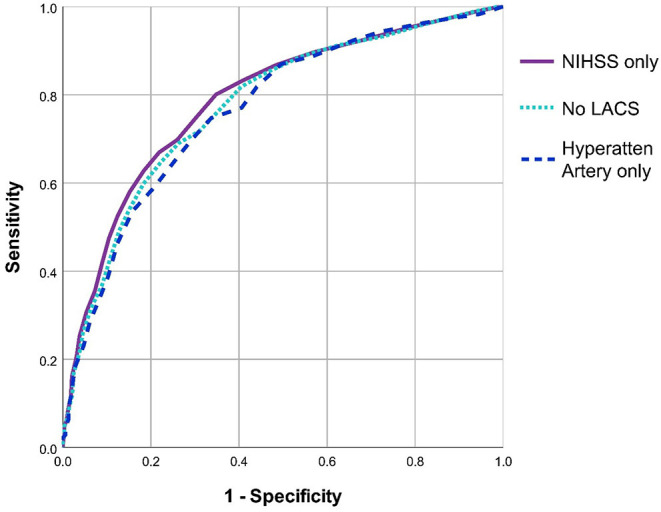
Methods: With data from the Third International Stroke Trial (IST-3, a large randomized-controlled trial of intravenous alteplase for ischaemic stroke) we used receiver-operating characteristic analysis to find a baseline National Institutes of Health Stroke Scale (NIHSS) threshold for identifying patients who developed medium-large ischaemic lesions within 48 h. From patients with baseline CT (acquired <6 h from stroke onset), we used this NIHSS threshold for selection and tested whether favorable outcome after alteplase (6-month Oxford Handicap Score 0-2) differed between patients with NAIBT vs. with those with visible lesions on baseline CT using binary logistic regression (controlled for age, NIHSS, time from stroke onset to CT).
Results: From 2,961 patients (median age 81 years, median 2.6 h from stroke onset, 1,534 [51.8%] female, 1,484 [50.1%] allocated alteplase), NIHSS>11 best identified those with medium-large ischaemic lesions (area under curve = 0.79, sensitivity = 72.3%, specificity = 71.9%). In IST-3, 1,404/2,961 (47.4%) patients had baseline CT and NIHSS>11. Of these, 745/1,404 (53.1%) had visible baseline ischaemic lesions, 659/1,404 (46.9%) did not (NAIBT). Adjusted odds ratio for favorable outcome after alteplase was 1.54 (95% confidence interval, 1.01-2.36), p = 0.045 among patients with NAIBT vs. 1.61 (0.97-2.67), p = 0.066 for patients with visible lesions, with no evidence of an alteplase-NAIBT interaction (p-value = 0.895).
Conclusions: Patients with ischaemic stroke and NIHSS >11 commonly develop sizeable ischaemic brain lesions by 48 h that may not be visible within 6 h of stroke onset. Invisible ischaemic lesions may indicate tissue viability. In IST-3, patients with this clinical-radiological mismatch allocated to alteplase achieved more favorable outcome than those allocated to control.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
