{"title":"The use of preoperative inferior vena cava ultrasound to predict anaesthesia-induced hypotension: a systematic review.","authors":"Sumit Roy Chowdhury, Priyankar Kumar Datta, Souvik Maitra, Dimple Rawat, Dalim Kumar Baidya, Avishek Roy, Sayan Nath","doi":"10.5114/ait.2023.125310","DOIUrl":null,"url":null,"abstract":"<p><p>Preoperative ultrasound assessment of inferior vena cava (IVC) diameter and the collapsi-bility index might identify patients with intravascular volume depletion. The purpose of this review was to gather the existing evidence to find out whether preoperative IVC ultrasound (IVCUS) derived parameters can reliably predict hypotension after spinal or general anaesthesia. PubMed was searched to identify research articles that addressed the role of IVC ultrasound in predicting hypotension after spinal and general anaesthesia in adult patients. We included 4 randomized control trials and 17 observational studies in our final review. Among these, 15 studies involved spinal anaesthesia and 6 studies involved general anaesthesia. Heterogeneity with respect to the patient populations under evaluation, definitions used for hypotension after anaesthesia, IVCUS assessment methods, and cut-off values for IVCUS-derived parameters to predict hypotension precluded pooled meta-analysis. The maximum and minimum reported sensitivity of the IVC collapsibility index (IVCCI) for predicting post-spinal hypotension was 84.6% and 58.8% respectively, while the maximum and minimum specificities were 93.1% and 23.5% respectively. For the prediction of hypotension after general anaesthesia induction, the reported ranges of sensitivity and specificity of IVCCI were 86.67% to 45.5% and 94.29% to 77.27%, respectively. Current literature on the predictive role of IVCUS for hypotension after anaesthesia is heterogeneous both in methodology and in results. Standardization of the definition of hypotension under anaesthesia, method of IVCUS assessment, and the cut-offs for IVC diameter and the collapsibility index for prediction of hypotension after anaesthesia are necessary for drawing clinically relevant conclusions.</p>","PeriodicalId":7750,"journal":{"name":"Anaesthesiology intensive therapy","volume":"55 1","pages":"18-31"},"PeriodicalIF":1.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/87/5c/AIT-55-50184.PMC10156560.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anaesthesiology intensive therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/ait.2023.125310","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
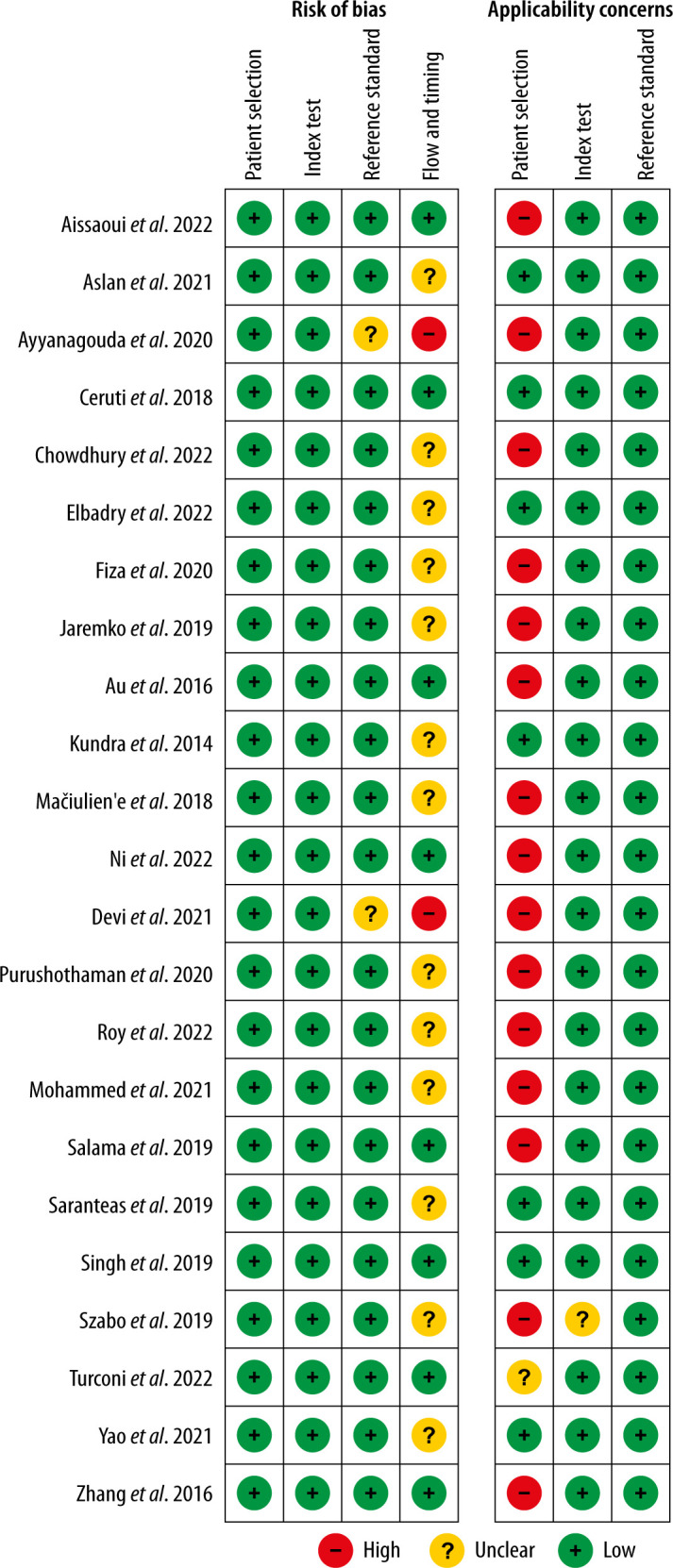
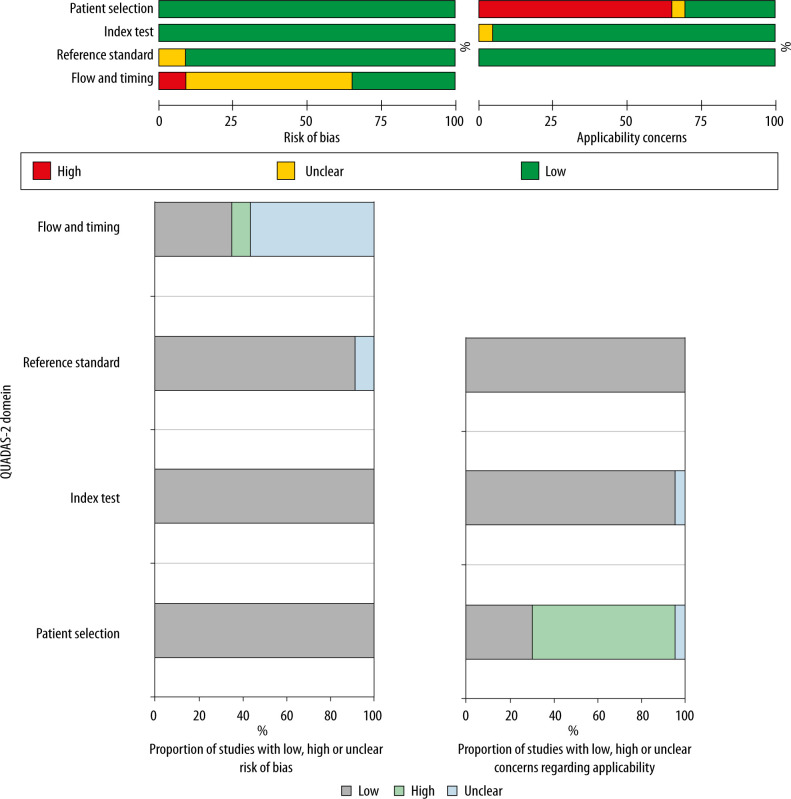
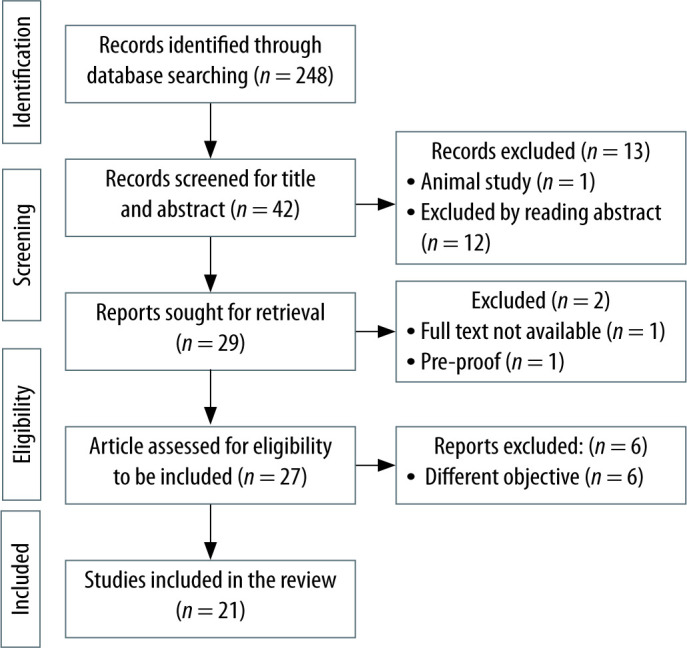
Preoperative ultrasound assessment of inferior vena cava (IVC) diameter and the collapsi-bility index might identify patients with intravascular volume depletion. The purpose of this review was to gather the existing evidence to find out whether preoperative IVC ultrasound (IVCUS) derived parameters can reliably predict hypotension after spinal or general anaesthesia. PubMed was searched to identify research articles that addressed the role of IVC ultrasound in predicting hypotension after spinal and general anaesthesia in adult patients. We included 4 randomized control trials and 17 observational studies in our final review. Among these, 15 studies involved spinal anaesthesia and 6 studies involved general anaesthesia. Heterogeneity with respect to the patient populations under evaluation, definitions used for hypotension after anaesthesia, IVCUS assessment methods, and cut-off values for IVCUS-derived parameters to predict hypotension precluded pooled meta-analysis. The maximum and minimum reported sensitivity of the IVC collapsibility index (IVCCI) for predicting post-spinal hypotension was 84.6% and 58.8% respectively, while the maximum and minimum specificities were 93.1% and 23.5% respectively. For the prediction of hypotension after general anaesthesia induction, the reported ranges of sensitivity and specificity of IVCCI were 86.67% to 45.5% and 94.29% to 77.27%, respectively. Current literature on the predictive role of IVCUS for hypotension after anaesthesia is heterogeneous both in methodology and in results. Standardization of the definition of hypotension under anaesthesia, method of IVCUS assessment, and the cut-offs for IVC diameter and the collapsibility index for prediction of hypotension after anaesthesia are necessary for drawing clinically relevant conclusions.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
