Influence of Proximal Humeral Cortical Bone Thickness on the Radiographic Outcome After Osteosynthesis of Proximal Humeral Fractures: Propensity Matching Score Analysis.
{"title":"Influence of Proximal Humeral Cortical Bone Thickness on the Radiographic Outcome After Osteosynthesis of Proximal Humeral Fractures: Propensity Matching Score Analysis.","authors":"Ryogo Furuhata, Atsushi Tanji, Satoshi Oki, Yusaku Kamata","doi":"10.1177/21514593231198645","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Osteoporosis can affect the surgical outcomes of proximal humeral fractures in older people. Recently, the cortical bone thickness of the proximal humerus on plain radiograph has been proposed to reflect local osteoporosis of the proximal humerus; however, its effect on the surgical outcome of proximal humeral fractures remains unclear. The purpose of this study is to investigate the influence of cortical bone thickness on postoperative radiographic outcomes after osteosynthesis for proximal humeral fractures.</p><p><strong>Materials and methods: </strong>We retrospectively identified 190 patients (≥50 years) who underwent osteosynthesis with an intramedullary nail or plate for proximal humeral fractures. The patients were categorized into 2 groups according to the cut-off value of an average proximal humerus cortical bone thickness of 6 mm on plain radiographs: patients with and without local osteoporosis. After propensity score matching, we compared the incidence of postoperative radiographic complications between the 2 groups. We also performed subgroup analyses of outcomes in a subgroup of patients who underwent intramedullary nailing and those who underwent plate fixation.</p><p><strong>Results: </strong>Propensity score matching yielded 60 patients in each group. No significant difference in complication rates was observed between the 2 groups. However, in the intramedullary nailing subgroup, the incidence of reduction loss was significantly higher in patients with local osteoporosis than in those without local osteoporosis (51.7% vs 14.3%, <i>P</i> = .002).</p><p><strong>Discussion: </strong>The proximal humeral cortical bone thickness had no significant effect on the overall radiographic outcome; however, reduction loss after intramedullary nailing was susceptible to local osteoporosis of the proximal humerus.</p><p><strong>Conclusion: </strong>Our study suggests that plate fixation is advantageous in preventing postoperative reduction loss in patients with lower cortical bone thickness.</p>","PeriodicalId":48568,"journal":{"name":"Geriatric Orthopaedic Surgery & Rehabilitation","volume":"14 ","pages":"21514593231198645"},"PeriodicalIF":1.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5c/48/10.1177_21514593231198645.PMC10460996.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Geriatric Orthopaedic Surgery & Rehabilitation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/21514593231198645","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
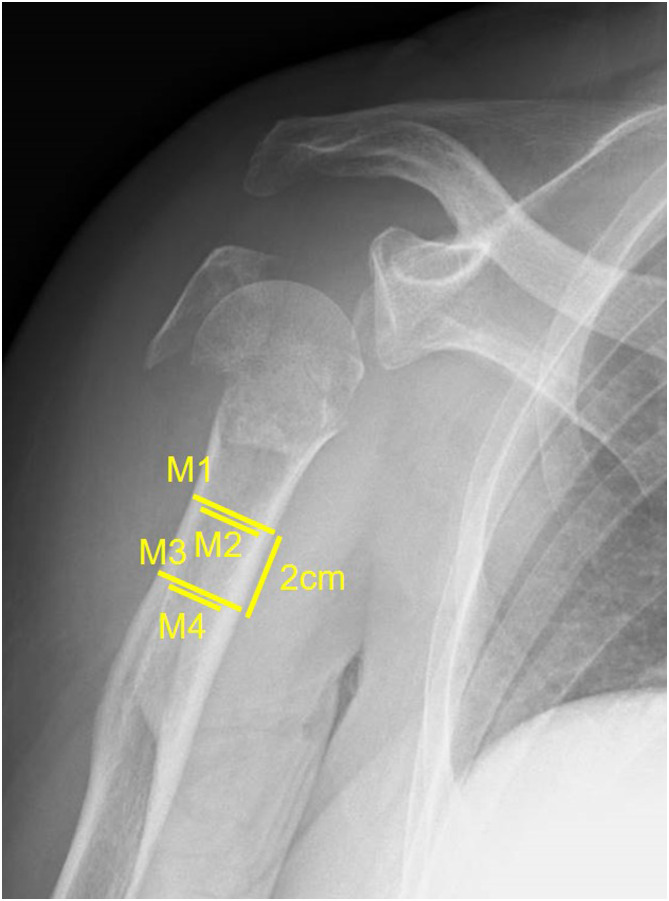
Introduction: Osteoporosis can affect the surgical outcomes of proximal humeral fractures in older people. Recently, the cortical bone thickness of the proximal humerus on plain radiograph has been proposed to reflect local osteoporosis of the proximal humerus; however, its effect on the surgical outcome of proximal humeral fractures remains unclear. The purpose of this study is to investigate the influence of cortical bone thickness on postoperative radiographic outcomes after osteosynthesis for proximal humeral fractures.
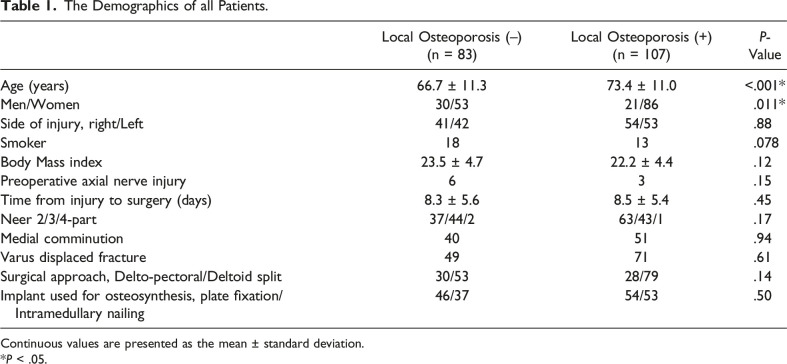
Materials and methods: We retrospectively identified 190 patients (≥50 years) who underwent osteosynthesis with an intramedullary nail or plate for proximal humeral fractures. The patients were categorized into 2 groups according to the cut-off value of an average proximal humerus cortical bone thickness of 6 mm on plain radiographs: patients with and without local osteoporosis. After propensity score matching, we compared the incidence of postoperative radiographic complications between the 2 groups. We also performed subgroup analyses of outcomes in a subgroup of patients who underwent intramedullary nailing and those who underwent plate fixation.
Results: Propensity score matching yielded 60 patients in each group. No significant difference in complication rates was observed between the 2 groups. However, in the intramedullary nailing subgroup, the incidence of reduction loss was significantly higher in patients with local osteoporosis than in those without local osteoporosis (51.7% vs 14.3%, P = .002).
Discussion: The proximal humeral cortical bone thickness had no significant effect on the overall radiographic outcome; however, reduction loss after intramedullary nailing was susceptible to local osteoporosis of the proximal humerus.
Conclusion: Our study suggests that plate fixation is advantageous in preventing postoperative reduction loss in patients with lower cortical bone thickness.
骨质疏松症会影响老年人肱骨近端骨折的手术结果。最近,x线平片上肱骨近端皮质骨厚度被认为可以反映肱骨近端局部骨质疏松;然而,其对肱骨近端骨折手术结果的影响尚不清楚。本研究的目的是探讨皮质骨厚度对肱骨近端骨折植骨术后影像学结果的影响。材料和方法:我们回顾性研究了190例(≥50岁)肱骨近端骨折行髓内钉或钢板内固定的患者。根据x线平片肱骨近端皮质骨平均厚度6 mm的临界值将患者分为有和无局部骨质疏松症两组。倾向评分匹配后,我们比较了两组患者术后放射并发症的发生率。我们还对接受髓内钉和钢板固定的亚组患者进行了亚组结果分析。结果:倾向评分匹配每组60例。两组患者并发症发生率无显著差异。然而,在髓内钉亚组中,有局部骨质疏松的患者复位损失发生率明显高于无局部骨质疏松的患者(51.7% vs 14.3%, P = 0.002)。讨论:肱骨近端皮质骨厚度对整体影像学结果无显著影响;然而,髓内钉后复位损失容易导致肱骨近端局部骨质疏松。结论:我们的研究表明,钢板固定有利于防止皮质骨厚度较低的患者术后复位损失。
期刊介绍:
Geriatric Orthopaedic Surgery & Rehabilitation (GOS) is an open access, peer-reviewed journal that provides clinical information concerning musculoskeletal conditions affecting the aging population. GOS focuses on care of geriatric orthopaedic patients and their subsequent rehabilitation. This journal is a member of the Committee on Publication Ethics (COPE).




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
