Utility and optimal cut-off point of the Somatic Symptom Scale-8 for central sensitization syndrome among outpatients with somatic symptoms and related disorders.
{"title":"Utility and optimal cut-off point of the Somatic Symptom Scale-8 for central sensitization syndrome among outpatients with somatic symptoms and related disorders.","authors":"Kazuaki Hashimoto, Takeaki Takeuchi, Miki Hiiragi, Akiko Koyama, Yuzo Nakamura, Masahiro Hashizume","doi":"10.1186/s13030-022-00253-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Central sensitization syndrome (CSS) involves severe functional symptoms due to central sensitization. for patients with severe somatic symptoms and related disorders (SSRDs), central sensitization may be responsible for their functional symptoms. We hypothesized that screening for CSS in patients with SSRDs would identify those with severe disease. The Somatic Symptom Scale-8 (SSS-8) is a simple tool to assess medical conditions related to SSRDs, but the cut-off point to identify severe cases of comorbid CSS is unknown. This study aimed to determine the optimal cut-off point of SSS-8 for screening the CSS of patients with severe SSRDs.</p><p><strong>Methods: </strong>In total, 143 patients with SSRDs attending outpatient clinics of a university hospital in Japan were included in the study. The participants were evaluated using the SSS-8 for somatic symptoms, Hospital Anxiety and Depression Scale (HADS) for anxiety and depressive symptoms, Pain Catastrophizing Scale (PCS) for catastrophic thoughts, and Central Sensitization Inventory (CSI-A, B) for CSS. Receiver operating characteristic (ROC) curve analysis was performed using the propensity score. The area under the curve (AUC) was calculated using a propensity score considering PCS, age, sex, HADS, and CSI-B as confounders of SSS-8 and CSS to evaluate differences in diagnostic accuracy between patients with and without SSS-8. The sensitivity and specificity of the ROC analysis were then used to determine the cut-off point for discriminating severe cases of SSS-8.</p><p><strong>Results: </strong>Of the 143 participants, 126 responded (51 CSS group and 75 non-CSS group), with a valid response rate of 88.1 percent. In the ROC analysis, the propensity score including SSS-8 was statistically more accurate. The optimal cut-off point was 13, with an AUC of 0.88, sensitivity of 84.3 percent, and specificity of 77.3 percent.</p><p><strong>Conclusions: </strong>The SSS-8 is a useful tool for discriminating severe cases of SSRDs comorbid with CSS.</p>","PeriodicalId":9027,"journal":{"name":"BioPsychoSocial Medicine","volume":"16 1","pages":"24"},"PeriodicalIF":2.4000,"publicationDate":"2022-11-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9694559/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BioPsychoSocial Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13030-022-00253-2","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Central sensitization syndrome (CSS) involves severe functional symptoms due to central sensitization. for patients with severe somatic symptoms and related disorders (SSRDs), central sensitization may be responsible for their functional symptoms. We hypothesized that screening for CSS in patients with SSRDs would identify those with severe disease. The Somatic Symptom Scale-8 (SSS-8) is a simple tool to assess medical conditions related to SSRDs, but the cut-off point to identify severe cases of comorbid CSS is unknown. This study aimed to determine the optimal cut-off point of SSS-8 for screening the CSS of patients with severe SSRDs.
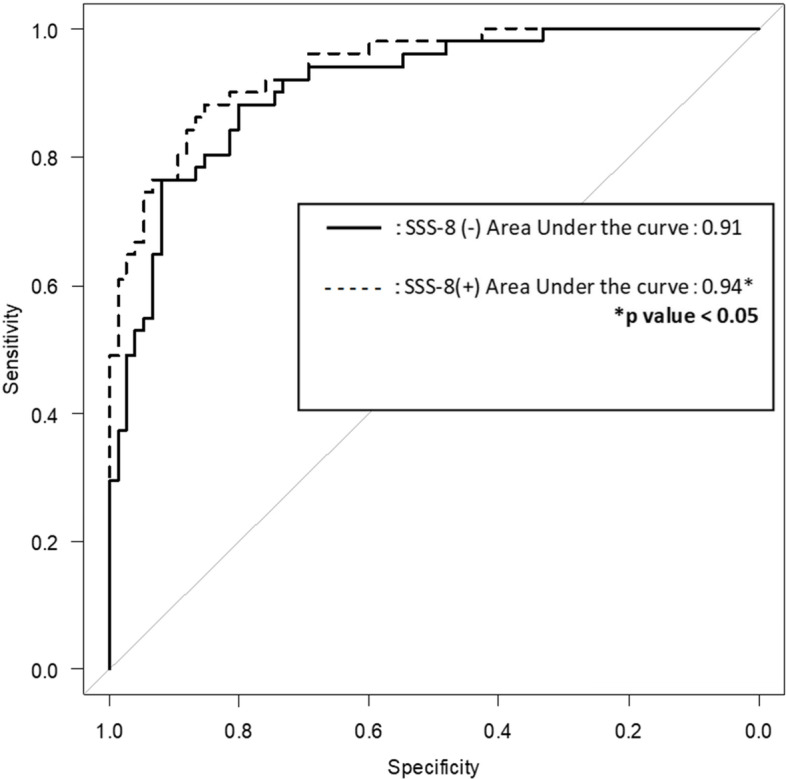
Methods: In total, 143 patients with SSRDs attending outpatient clinics of a university hospital in Japan were included in the study. The participants were evaluated using the SSS-8 for somatic symptoms, Hospital Anxiety and Depression Scale (HADS) for anxiety and depressive symptoms, Pain Catastrophizing Scale (PCS) for catastrophic thoughts, and Central Sensitization Inventory (CSI-A, B) for CSS. Receiver operating characteristic (ROC) curve analysis was performed using the propensity score. The area under the curve (AUC) was calculated using a propensity score considering PCS, age, sex, HADS, and CSI-B as confounders of SSS-8 and CSS to evaluate differences in diagnostic accuracy between patients with and without SSS-8. The sensitivity and specificity of the ROC analysis were then used to determine the cut-off point for discriminating severe cases of SSS-8.
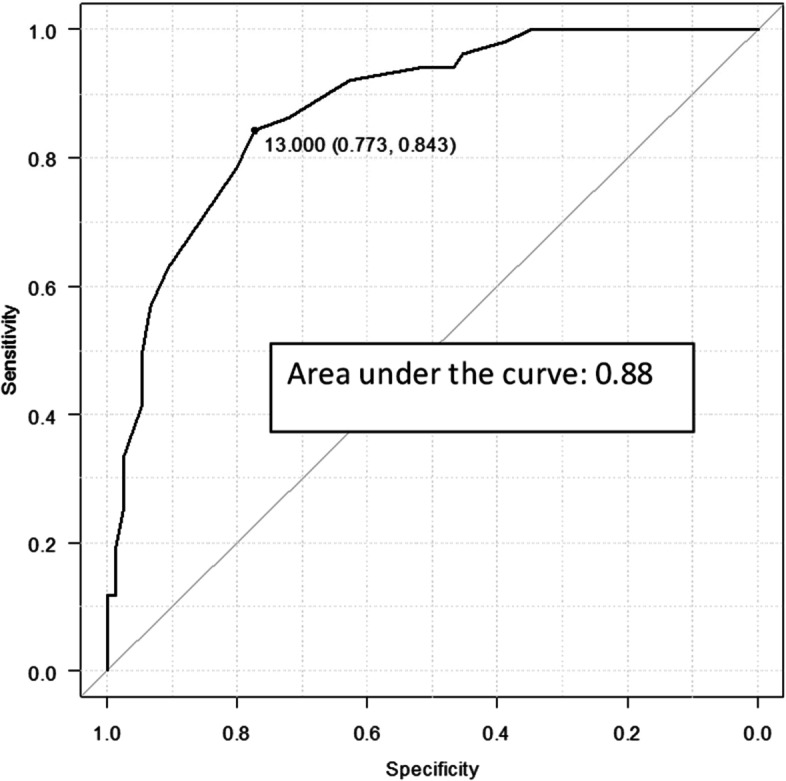
Results: Of the 143 participants, 126 responded (51 CSS group and 75 non-CSS group), with a valid response rate of 88.1 percent. In the ROC analysis, the propensity score including SSS-8 was statistically more accurate. The optimal cut-off point was 13, with an AUC of 0.88, sensitivity of 84.3 percent, and specificity of 77.3 percent.
Conclusions: The SSS-8 is a useful tool for discriminating severe cases of SSRDs comorbid with CSS.
期刊介绍:
BioPsychoSocial Medicine is an open access, peer-reviewed online journal that encompasses all aspects of the interrelationships between the biological, psychological, social, and behavioral factors of health and illness. BioPsychoSocial Medicine is the official journal of the Japanese Society of Psychosomatic Medicine, and publishes research on psychosomatic disorders and diseases that are characterized by objective organic changes and/or functional changes that could be induced, progressed, aggravated, or exacerbated by psychological, social, and/or behavioral factors and their associated psychosomatic treatments.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
