Raymond J. Strobel MD, MSc , Eric J. Charles MD, PhD , J. Hunter Mehaffey MD, MSc , Robert B. Hawkins MD, MSc , Mohammed A. Quader MD , Jeffrey B. Rich MD , Alan M. Speir MD , Gorav Ailawadi MD, MBA , Investigators for the Virginia Cardiac Services Quality Initiative
{"title":"Effect of Socioeconomic Distress on Risk-Adjusted Mortality After Valve Surgery for Infective Endocarditis","authors":"Raymond J. Strobel MD, MSc , Eric J. Charles MD, PhD , J. Hunter Mehaffey MD, MSc , Robert B. Hawkins MD, MSc , Mohammed A. Quader MD , Jeffrey B. Rich MD , Alan M. Speir MD , Gorav Ailawadi MD, MBA , Investigators for the Virginia Cardiac Services Quality Initiative","doi":"10.1053/j.semtcvs.2022.05.007","DOIUrl":null,"url":null,"abstract":"<div><p><span>Infective endocarditis<span> affects patients of all socioeconomic status. We hypothesized that the Distressed Communities Index (DCI), a comprehensive assessment of socioeconomic status, would be associated with risk-adjusted mortality for patients with endocarditis. All patients with endocarditis (2001-2017) in a regional Society of Thoracic Surgeons database were analyzed. DCI scores range from 0 (no socioeconomic distress) to 100 (severe distress) and account for unemployment, poverty rate, median income, housing vacancies, education level, and business growth by zip code. The most distressed patients (top quartile, DCI > 75) were compared to all other patients. Hierarchical logistic regression<span> modeled the association between DCI and mortality. A total of 2,075 patients were included (median age 55 years, 65.2% urgent/emergent cases, 42.7% self-pay). Major morbidity was 32.8% and operative mortality was 9.5%. Tricuspid/pulmonic valve endocarditis was present in 12.5% of cases, with significantly worse mean DCI compared to patients with left-sided endocarditis (median 55.3, IQR 20.3-77.6 vs 46.8, IQR 17.3-74.2, </span></span></span><em>P</em> = 0.016). High socioeconomic distress (DCI > 75) was associated with higher rates of major morbidity, operative mortality, increased length of stay, and higher total cost. After risk-adjustment, DCI was independently predictive of higher operative mortality for patients with endocarditis (OR 1.24 per DCI quartile increase, 95% CI 1.06-1.45, <em>P</em> < 0.001). Increasing DCI, an indicator of poor socioeconomic status, independently predicts increased risk-adjusted mortality and resource utilization for patients with endocarditis. Accounting for socioeconomic status allows for more accurate risk prediction and resource allocation for patients with endocarditis.</p></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"35 3","pages":"Pages 497-507"},"PeriodicalIF":2.5000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1043067922001253","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/5/16 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 3
Abstract
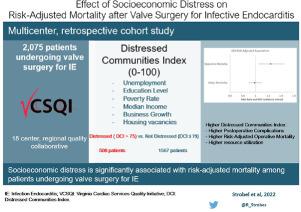
Infective endocarditis affects patients of all socioeconomic status. We hypothesized that the Distressed Communities Index (DCI), a comprehensive assessment of socioeconomic status, would be associated with risk-adjusted mortality for patients with endocarditis. All patients with endocarditis (2001-2017) in a regional Society of Thoracic Surgeons database were analyzed. DCI scores range from 0 (no socioeconomic distress) to 100 (severe distress) and account for unemployment, poverty rate, median income, housing vacancies, education level, and business growth by zip code. The most distressed patients (top quartile, DCI > 75) were compared to all other patients. Hierarchical logistic regression modeled the association between DCI and mortality. A total of 2,075 patients were included (median age 55 years, 65.2% urgent/emergent cases, 42.7% self-pay). Major morbidity was 32.8% and operative mortality was 9.5%. Tricuspid/pulmonic valve endocarditis was present in 12.5% of cases, with significantly worse mean DCI compared to patients with left-sided endocarditis (median 55.3, IQR 20.3-77.6 vs 46.8, IQR 17.3-74.2, P = 0.016). High socioeconomic distress (DCI > 75) was associated with higher rates of major morbidity, operative mortality, increased length of stay, and higher total cost. After risk-adjustment, DCI was independently predictive of higher operative mortality for patients with endocarditis (OR 1.24 per DCI quartile increase, 95% CI 1.06-1.45, P < 0.001). Increasing DCI, an indicator of poor socioeconomic status, independently predicts increased risk-adjusted mortality and resource utilization for patients with endocarditis. Accounting for socioeconomic status allows for more accurate risk prediction and resource allocation for patients with endocarditis.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
