Daniel S Rubin, Sylvia L Ranjeva, Jacek K Urbanek, Marta Karas, Maria Lucia L Madariaga, Megan Huisingh-Scheetz
{"title":"Smartphone-Based Gait Cadence to Identify Older Adults with Decreased Functional Capacity.","authors":"Daniel S Rubin, Sylvia L Ranjeva, Jacek K Urbanek, Marta Karas, Maria Lucia L Madariaga, Megan Huisingh-Scheetz","doi":"10.1159/000525344","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Functional capacity assessment is a critical step in the preoperative evaluation to identify patients at increased risk of cardiac complications and disability after major noncardiac surgery. Smartphones offer the potential to objectively measure functional capacity but are limited by inaccuracy in patients with poor functional capacity. Open-source methods exist to analyze accelerometer data to estimate gait cadence (steps/min), which is directly associated with activity intensity. Here, we used an updated Step Test smartphone application with an open-source method to analyze accelerometer data to estimate gait cadence and functional capacity in older adults.</p><p><strong>Methods: </strong>We performed a prospective observational cohort study within the Frailty, Activity, Body Composition and Energy Expenditure in Aging study at the University of Chicago. Participants completed the Duke Activity Status Index (DASI) and performed an in-clinic 6-min walk test (6MWT) while using the Step Test application on a study smartphone. Gait cadence was measured from the raw accelerometer data using an adaptive empirical pattern transformation method, which has been previously validated. A 6MWT distance of 370 m was used as an objective threshold to identify patients at high risk. We performed multivariable logistic regression to predict walking distance using a priori explanatory variables.</p><p><strong>Results: </strong>Sixty patients were enrolled in the study. Thirty-seven patients completed the protocol and were included in the final data analysis. The median (IQR) age of the overall cohort was 71 (69-74) years, with a body mass index of 31 (27-32). There were no differences in any clinical characteristics or functional measures between participants that were able to walk 370 m during the 6MWT and those that could not walk that distance. Median (IQR) gait cadence for the entire cohort was 110 (102-114) steps/min during the 6MWT. Median (IQR) gait cadence was higher in participants that walked more than 370 m during the 6MWT 112 (108-118) versus 106 (96-114) steps/min; <i>p</i> = 0.0157). The final multivariable model to identify participants that could not walk 370 m included only median gait cadence. The Youden's index cut-point was 107 steps/min with a sensitivity of 0.81 (95% CI: 0.77, 0.85) and a specificity of 0.57 (95% CI: 0.55, 0.59) and an AUCROC of 0.69 (95% CI: 0.51, 0.87).</p><p><strong>Conclusions: </strong>Our pilot study demonstrates the feasibility of using gait cadence as a measure to estimate functional capacity. Our study was limited by a smaller than expected sample size due to COVID-19, and thus, a prospective study with preoperative patients that measures outcomes is necessary to validate our findings.</p>","PeriodicalId":11242,"journal":{"name":"Digital Biomarkers","volume":"6 2","pages":"61-70"},"PeriodicalIF":0.0000,"publicationDate":"2022-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3a/3b/dib-0006-0061.PMC9386413.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digital Biomarkers","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000525344","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Computer Science","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Functional capacity assessment is a critical step in the preoperative evaluation to identify patients at increased risk of cardiac complications and disability after major noncardiac surgery. Smartphones offer the potential to objectively measure functional capacity but are limited by inaccuracy in patients with poor functional capacity. Open-source methods exist to analyze accelerometer data to estimate gait cadence (steps/min), which is directly associated with activity intensity. Here, we used an updated Step Test smartphone application with an open-source method to analyze accelerometer data to estimate gait cadence and functional capacity in older adults.
Methods: We performed a prospective observational cohort study within the Frailty, Activity, Body Composition and Energy Expenditure in Aging study at the University of Chicago. Participants completed the Duke Activity Status Index (DASI) and performed an in-clinic 6-min walk test (6MWT) while using the Step Test application on a study smartphone. Gait cadence was measured from the raw accelerometer data using an adaptive empirical pattern transformation method, which has been previously validated. A 6MWT distance of 370 m was used as an objective threshold to identify patients at high risk. We performed multivariable logistic regression to predict walking distance using a priori explanatory variables.
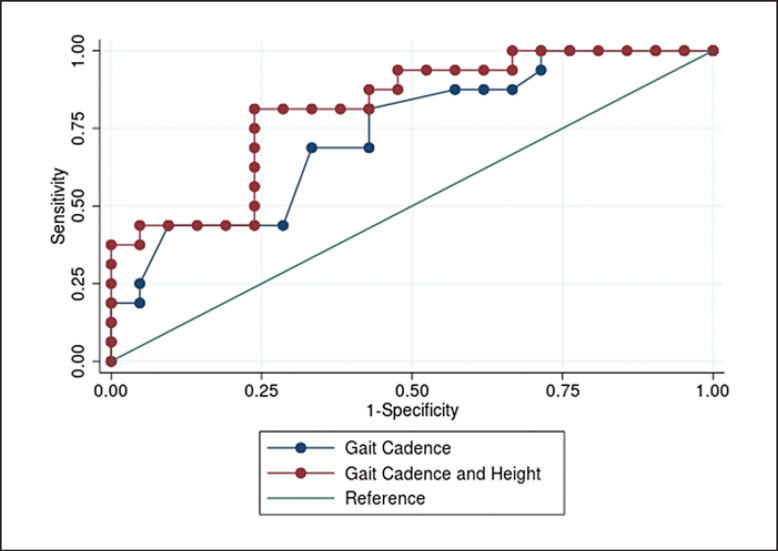
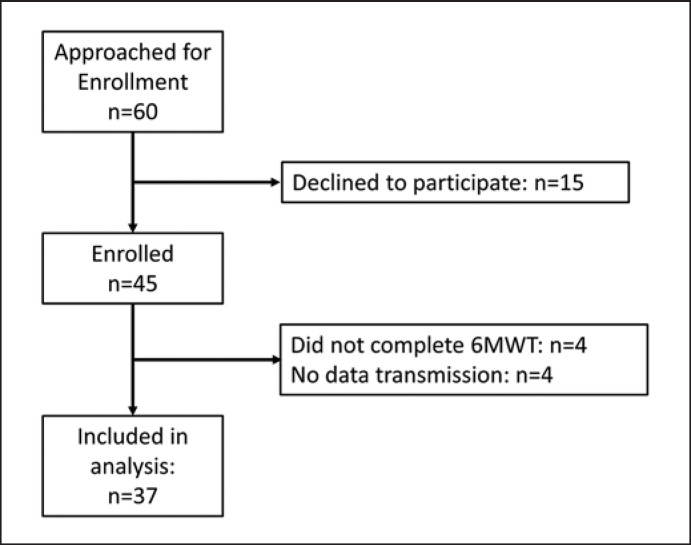
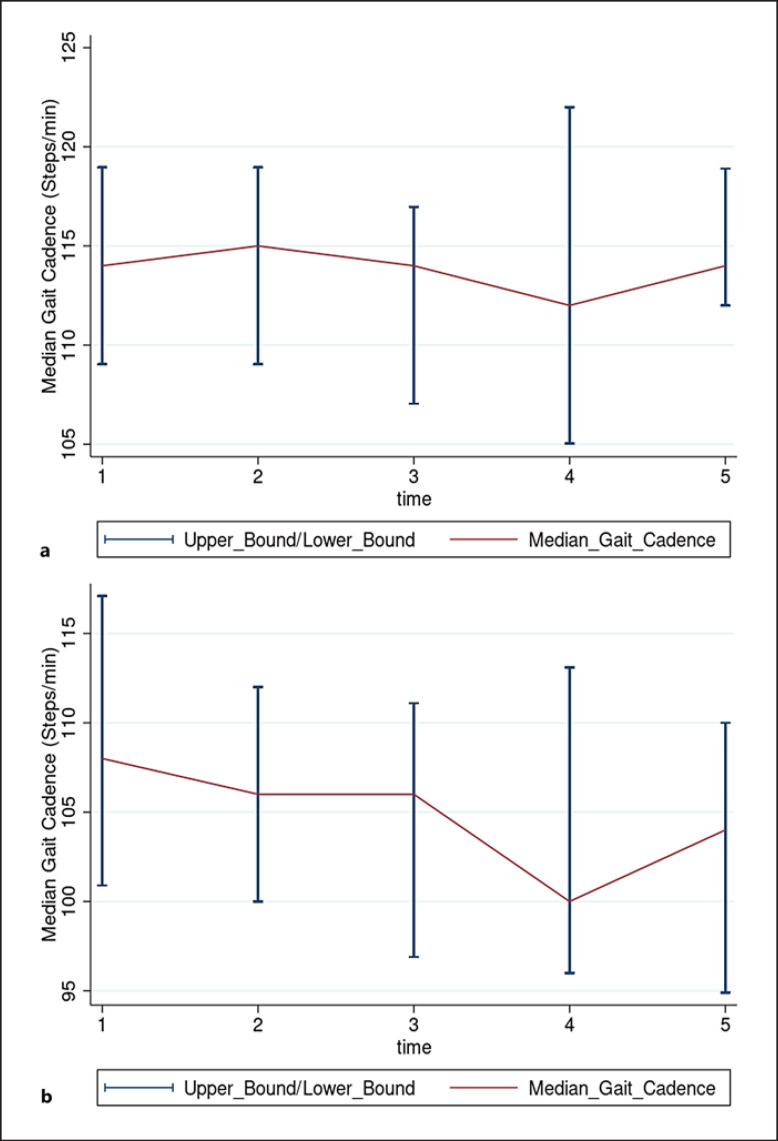
Results: Sixty patients were enrolled in the study. Thirty-seven patients completed the protocol and were included in the final data analysis. The median (IQR) age of the overall cohort was 71 (69-74) years, with a body mass index of 31 (27-32). There were no differences in any clinical characteristics or functional measures between participants that were able to walk 370 m during the 6MWT and those that could not walk that distance. Median (IQR) gait cadence for the entire cohort was 110 (102-114) steps/min during the 6MWT. Median (IQR) gait cadence was higher in participants that walked more than 370 m during the 6MWT 112 (108-118) versus 106 (96-114) steps/min; p = 0.0157). The final multivariable model to identify participants that could not walk 370 m included only median gait cadence. The Youden's index cut-point was 107 steps/min with a sensitivity of 0.81 (95% CI: 0.77, 0.85) and a specificity of 0.57 (95% CI: 0.55, 0.59) and an AUCROC of 0.69 (95% CI: 0.51, 0.87).
Conclusions: Our pilot study demonstrates the feasibility of using gait cadence as a measure to estimate functional capacity. Our study was limited by a smaller than expected sample size due to COVID-19, and thus, a prospective study with preoperative patients that measures outcomes is necessary to validate our findings.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
