{"title":"Vasoplegic Syndrome and Anaesthesia: A Narrative Review.","authors":"Begüm Nemika Gökdemir, Nedim Çekmen","doi":"10.4274/TJAR.2023.221093","DOIUrl":null,"url":null,"abstract":"<p><p>Vasoplegic syndrome (VS) is defined as low systemic vascular resistance, normal or high cardiac output, and resistant hypotension unresponsive to vasopressor agents and intravenous volume. VS is a frequently encountered complication in cardiovascular and transplantation surgery, burns, trauma, pancreatitis, and sepsis. The basis of the pathophysiology is associated with an imbalance of vasodilator and vasoconstrictive structure in vascular smooth muscle cells and is highly complex. The pathogenesis of VS has several mechanisms, including overproduction of iNO, stimulation of ATP-dependent K+ channels and NF-κB, and vasopressin receptor 1A (V1A-receptor) down-regulation. Available treatments involve volume and inotropes administration, vasopressin, methylene blue, hydroxocobalamin, Ca++, vitamin C, and thiamine, and should also restore vascular tone and improve vasoplegia. Other treatments could include angiotensin II, corticosteroids, NF-κB inhibitor, ATP-dependent K+ channel blocker, indigo carmine, and hyperbaric oxygen therapy. Despite modern advances in treatment, the mortality rate is still 30-50%. It is challenging for an anaesthesiologist to consider this syndrome's diagnosis and manage its treatment. Our review aims to review the diagnosis, predisposing factors, pathophysiology, treatment, and anaesthesia approach of VS during anaesthesia and to suggest a treatment algorithm.</p>","PeriodicalId":23353,"journal":{"name":"Turkish journal of anaesthesiology and reanimation","volume":"51 4","pages":"280-289"},"PeriodicalIF":0.9000,"publicationDate":"2023-08-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10440482/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Turkish journal of anaesthesiology and reanimation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4274/TJAR.2023.221093","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
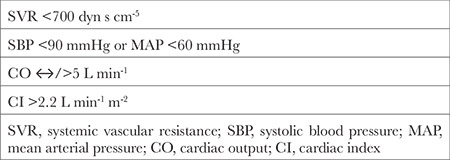
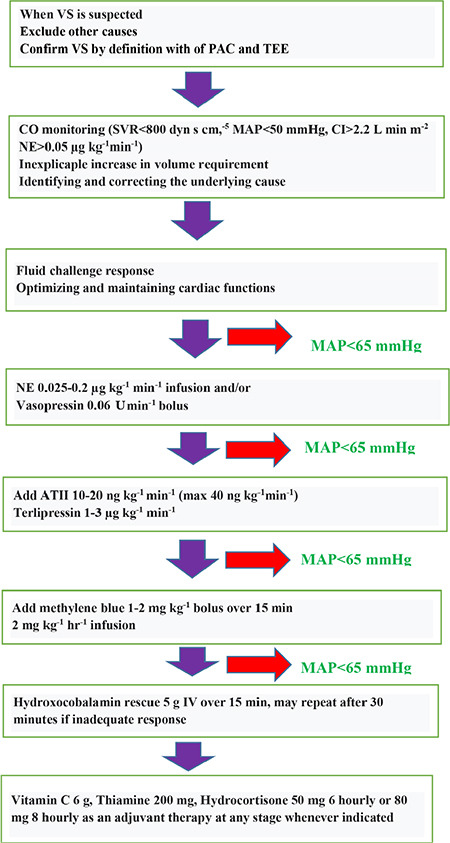
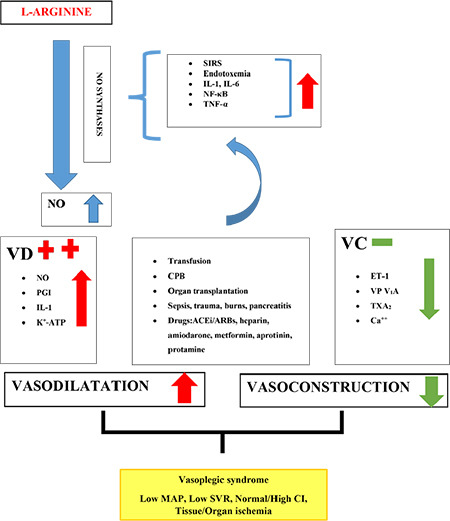
Vasoplegic syndrome (VS) is defined as low systemic vascular resistance, normal or high cardiac output, and resistant hypotension unresponsive to vasopressor agents and intravenous volume. VS is a frequently encountered complication in cardiovascular and transplantation surgery, burns, trauma, pancreatitis, and sepsis. The basis of the pathophysiology is associated with an imbalance of vasodilator and vasoconstrictive structure in vascular smooth muscle cells and is highly complex. The pathogenesis of VS has several mechanisms, including overproduction of iNO, stimulation of ATP-dependent K+ channels and NF-κB, and vasopressin receptor 1A (V1A-receptor) down-regulation. Available treatments involve volume and inotropes administration, vasopressin, methylene blue, hydroxocobalamin, Ca++, vitamin C, and thiamine, and should also restore vascular tone and improve vasoplegia. Other treatments could include angiotensin II, corticosteroids, NF-κB inhibitor, ATP-dependent K+ channel blocker, indigo carmine, and hyperbaric oxygen therapy. Despite modern advances in treatment, the mortality rate is still 30-50%. It is challenging for an anaesthesiologist to consider this syndrome's diagnosis and manage its treatment. Our review aims to review the diagnosis, predisposing factors, pathophysiology, treatment, and anaesthesia approach of VS during anaesthesia and to suggest a treatment algorithm.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
