Incidence and Factors Associated with Postspinal Headache in Obstetric Mothers Who Underwent Spinal Anesthesia from a Tertiary Hospital in Western Uganda: A Prospective Cohort Study.
Mohamud Jelle Osman, Joy Muhumuza, Yarine Fajardo, Andrew Kwikiriza, Baluku Asanairi, Rogers Kajabwangu, Marie Pascaline Sabine Ishimwe, Theoneste Hakizimana
{"title":"Incidence and Factors Associated with Postspinal Headache in Obstetric Mothers Who Underwent Spinal Anesthesia from a Tertiary Hospital in Western Uganda: A Prospective Cohort Study.","authors":"Mohamud Jelle Osman, Joy Muhumuza, Yarine Fajardo, Andrew Kwikiriza, Baluku Asanairi, Rogers Kajabwangu, Marie Pascaline Sabine Ishimwe, Theoneste Hakizimana","doi":"10.1155/2023/5522444","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The proportion of obstetric mothers reporting postspinal headache (PSH) in Uganda is high. The aim of this study is to determine the incidence and factors associated with postspinal headache among obstetric patients who underwent spinal anesthesia during cesarean section at a tertiary hospital in Western Uganda.</p><p><strong>Methods: </strong>A prospective cohort study was done on 274 consecutively enrolled obstetric patients at Fort Portal Regional Referral Hospital (FRRH) from August to November 2022. Pretested questionnaires were used to obtain the data needed for analysis. The data were entered into Microsoft Excel version 16, coded, and transported into SPSS version 22 for analysis. Descriptive statistics was used to determine the incidence of postspinal headache. Binary logistic regression was computed to obtain factors associated with postspinal headache.</p><p><strong>Results: </strong>The overall incidence of postspinal headache was 38.3% (95% CI: 32.5-44.4). Factors with higher odds of developing postspinal headache included using cutting needle (<sup>a</sup>OR 3.206, 95% CI: 1.408-7.299, <i>p</i>=0.006), having a previous history of chronic headache (aOR 3.326, 95% CI: 1.409-7.85, <i>p</i>=0.006), having lost >1500 mls of blood intraoperatively (<sup>a</sup>OR 6.618, 95% CI: 1.582-27.687, <i>p</i>=0.010), initiation of ambulation >24 h after spinal anesthesia (<sup>a</sup>OR 2.346, 95% CI: 1.079-5.102, <i>p</i>=0.032), allowing 2-3 drops of cerebrospinal fluid (CSF) to fall (aOR 3.278, 95% CI: 1.263-8.510, <i>p</i>=0.015), undergoing 2 puncture attempts (<sup>a</sup>OR 7.765, 95% CI: 3.48-17.326, <i>p</i> ≤ 0.001), 3 puncture attempts (<sup>a</sup>OR 27.61, 95% CI: 7.671-99.377, <i>p</i> ≤ 0.001) and >3 puncture attempts (<sup>a</sup>OR 20.17, 95% CI: 1.614-155.635, <i>p</i>=0.004), those prescribed weak opioids (<sup>a</sup>OR 20.745, 95% CI: 2.964-145.212, <i>p</i>=0.002), nonsteroidal anti-inflammatory drug (NSAID) with nonopioids (<sup>a</sup>OR 6.104, 95% CI: 1.257-29.651, <i>p</i>=0.025), and NSAID with weak opioids (<sup>a</sup>OR 5.149, 95% CI: 1.047-25.326, <i>p</i>=0.044). Women with a body mass index (BMI) of 25-29.9 kg/m<sup>2</sup> (<sup>a</sup>OR 0.471, 95% CI: 0.224-0.989, <i>p</i>=0.047) and a level of puncture entry at L3-4 (<sup>a</sup>OR 0.381, 95% CI: 0.167-0.868, <i>p</i>=0.022) had lower odds of developing PSH.</p><p><strong>Conclusions: </strong>The incidence of postspinal headache is still high as compared to the global range. This was significantly associated with needle design, amount of cerebro-spinal fluid lost, number of puncture attempts, body mass index, previous diagnosis with chronic headache, amount of intraoperative blood loss, time at start of ambulation, level of puncture entry, and class of analgesic prescribed. We recommend the use of a smaller gauge needle, preventing CSF loss, deliberate attempts to ensure successful puncture with fewer attempts, puncture attempts at L3-4, reducing intraoperative blood loss, earlier ambulation, and prescribing adequate analgesia to reduce the incidence of postspinal headache.</p>","PeriodicalId":7834,"journal":{"name":"Anesthesiology Research and Practice","volume":"2023 ","pages":"5522444"},"PeriodicalIF":1.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10435309/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesiology Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/5522444","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The proportion of obstetric mothers reporting postspinal headache (PSH) in Uganda is high. The aim of this study is to determine the incidence and factors associated with postspinal headache among obstetric patients who underwent spinal anesthesia during cesarean section at a tertiary hospital in Western Uganda.
Methods: A prospective cohort study was done on 274 consecutively enrolled obstetric patients at Fort Portal Regional Referral Hospital (FRRH) from August to November 2022. Pretested questionnaires were used to obtain the data needed for analysis. The data were entered into Microsoft Excel version 16, coded, and transported into SPSS version 22 for analysis. Descriptive statistics was used to determine the incidence of postspinal headache. Binary logistic regression was computed to obtain factors associated with postspinal headache.
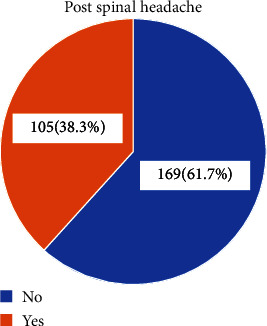
Results: The overall incidence of postspinal headache was 38.3% (95% CI: 32.5-44.4). Factors with higher odds of developing postspinal headache included using cutting needle (aOR 3.206, 95% CI: 1.408-7.299, p=0.006), having a previous history of chronic headache (aOR 3.326, 95% CI: 1.409-7.85, p=0.006), having lost >1500 mls of blood intraoperatively (aOR 6.618, 95% CI: 1.582-27.687, p=0.010), initiation of ambulation >24 h after spinal anesthesia (aOR 2.346, 95% CI: 1.079-5.102, p=0.032), allowing 2-3 drops of cerebrospinal fluid (CSF) to fall (aOR 3.278, 95% CI: 1.263-8.510, p=0.015), undergoing 2 puncture attempts (aOR 7.765, 95% CI: 3.48-17.326, p ≤ 0.001), 3 puncture attempts (aOR 27.61, 95% CI: 7.671-99.377, p ≤ 0.001) and >3 puncture attempts (aOR 20.17, 95% CI: 1.614-155.635, p=0.004), those prescribed weak opioids (aOR 20.745, 95% CI: 2.964-145.212, p=0.002), nonsteroidal anti-inflammatory drug (NSAID) with nonopioids (aOR 6.104, 95% CI: 1.257-29.651, p=0.025), and NSAID with weak opioids (aOR 5.149, 95% CI: 1.047-25.326, p=0.044). Women with a body mass index (BMI) of 25-29.9 kg/m2 (aOR 0.471, 95% CI: 0.224-0.989, p=0.047) and a level of puncture entry at L3-4 (aOR 0.381, 95% CI: 0.167-0.868, p=0.022) had lower odds of developing PSH.
Conclusions: The incidence of postspinal headache is still high as compared to the global range. This was significantly associated with needle design, amount of cerebro-spinal fluid lost, number of puncture attempts, body mass index, previous diagnosis with chronic headache, amount of intraoperative blood loss, time at start of ambulation, level of puncture entry, and class of analgesic prescribed. We recommend the use of a smaller gauge needle, preventing CSF loss, deliberate attempts to ensure successful puncture with fewer attempts, puncture attempts at L3-4, reducing intraoperative blood loss, earlier ambulation, and prescribing adequate analgesia to reduce the incidence of postspinal headache.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
