Leslie C.M. Johnson , Nancy J. Thompson , Mohammed K. Ali , Kirk Elifson , Lydia Chwastiak , Viswanathan Mohan , Ranjit Mohan Anjana , Subramani Poongothai , Nikhil Tandon
{"title":"A realist process evaluation of the INtegrating DEPrEssioN and Diabetes treatmENT (INDEPENDENT) randomized controlled trial in India","authors":"Leslie C.M. Johnson , Nancy J. Thompson , Mohammed K. Ali , Kirk Elifson , Lydia Chwastiak , Viswanathan Mohan , Ranjit Mohan Anjana , Subramani Poongothai , Nikhil Tandon","doi":"10.1016/j.ajmo.2022.100015","DOIUrl":null,"url":null,"abstract":"<div><h3>Aims</h3><p>We aimed to determine what key resources, mechanisms, and contextual factors are necessary to integrate depression and diabetes treatment into low-resource settings.</p></div><div><h3>Methods</h3><p>A realist evaluation framework was employed to conduct a comparative case study. Data were collected through document review, key informant interviews (<em>n</em>=4), activity logs, and interviews with implementing health care providers (n=11) to test and refine program theories for collaborative care.</p></div><div><h3>Results</h3><p>Efforts to enhance patient care coordination (i.e., adapting clinics’ patient flow and resources, on-going trainings, and on-site support for care coordinators) improved implementation of depression treatment by usual care diabetes physicians. Clinician's avoidance of the term depression was identified as a barrier to mental health counseling and treatment.</p></div><div><h3>Conclusions</h3><p>The variations in organizational features and processes linked to implementation activities across two clinics provided an opportunity to examine how and why different contextual factors help or hinder the implementation process. Findings from this study demonstrate that successful implementation of an integrated depression and diabetes care model is feasible in a low-resource setting, while the revised program theories provide an explanatory framework of coordinated care implementation processes that can inform future efforts to disseminate and scale this care model.</p></div>","PeriodicalId":72168,"journal":{"name":"American journal of medicine open","volume":"8 ","pages":"Article 100015"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ea/f0/nihms-1858340.PMC9788650.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American journal of medicine open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2667036422000097","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aims
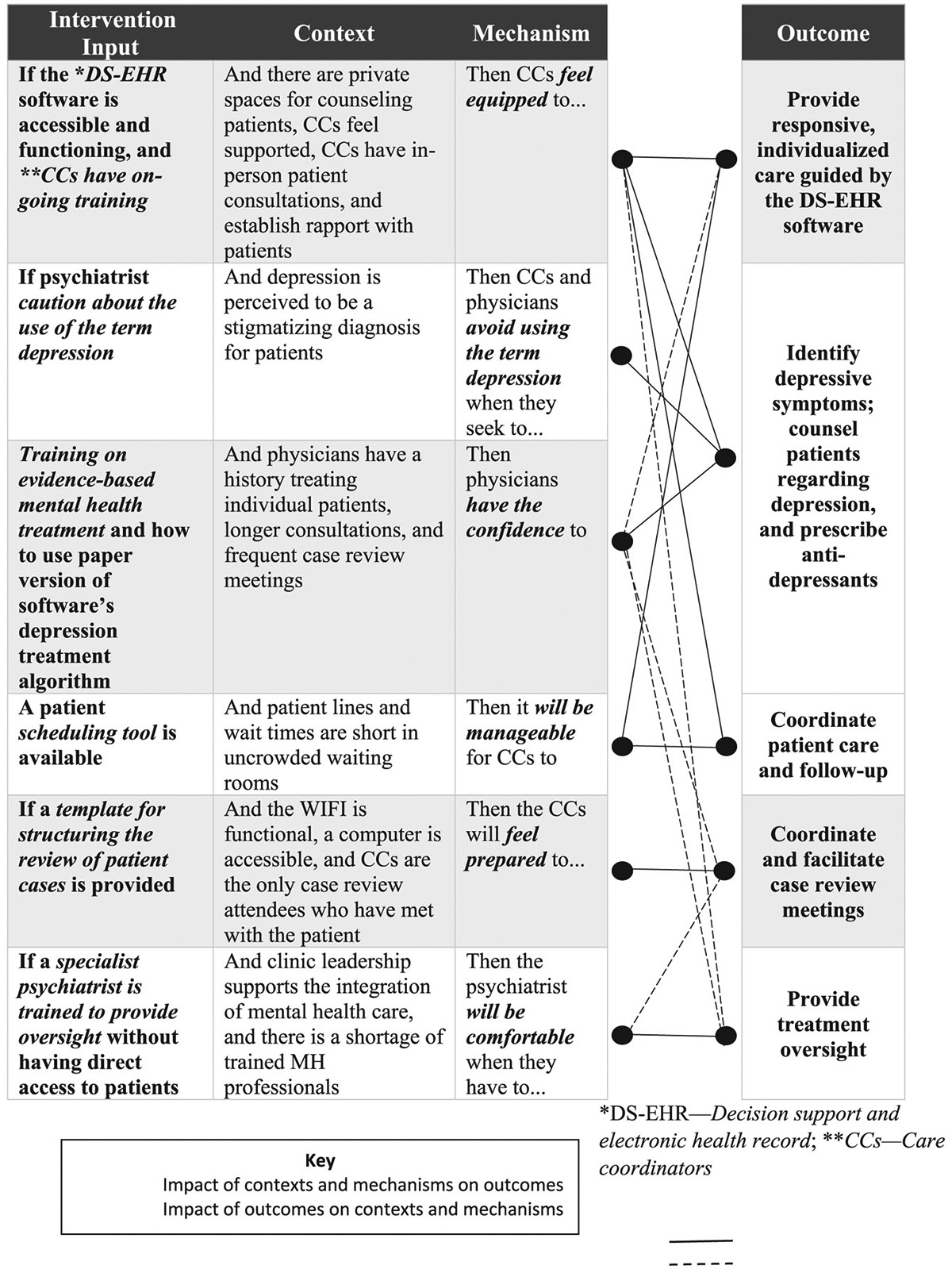
We aimed to determine what key resources, mechanisms, and contextual factors are necessary to integrate depression and diabetes treatment into low-resource settings.
Methods
A realist evaluation framework was employed to conduct a comparative case study. Data were collected through document review, key informant interviews (n=4), activity logs, and interviews with implementing health care providers (n=11) to test and refine program theories for collaborative care.
Results
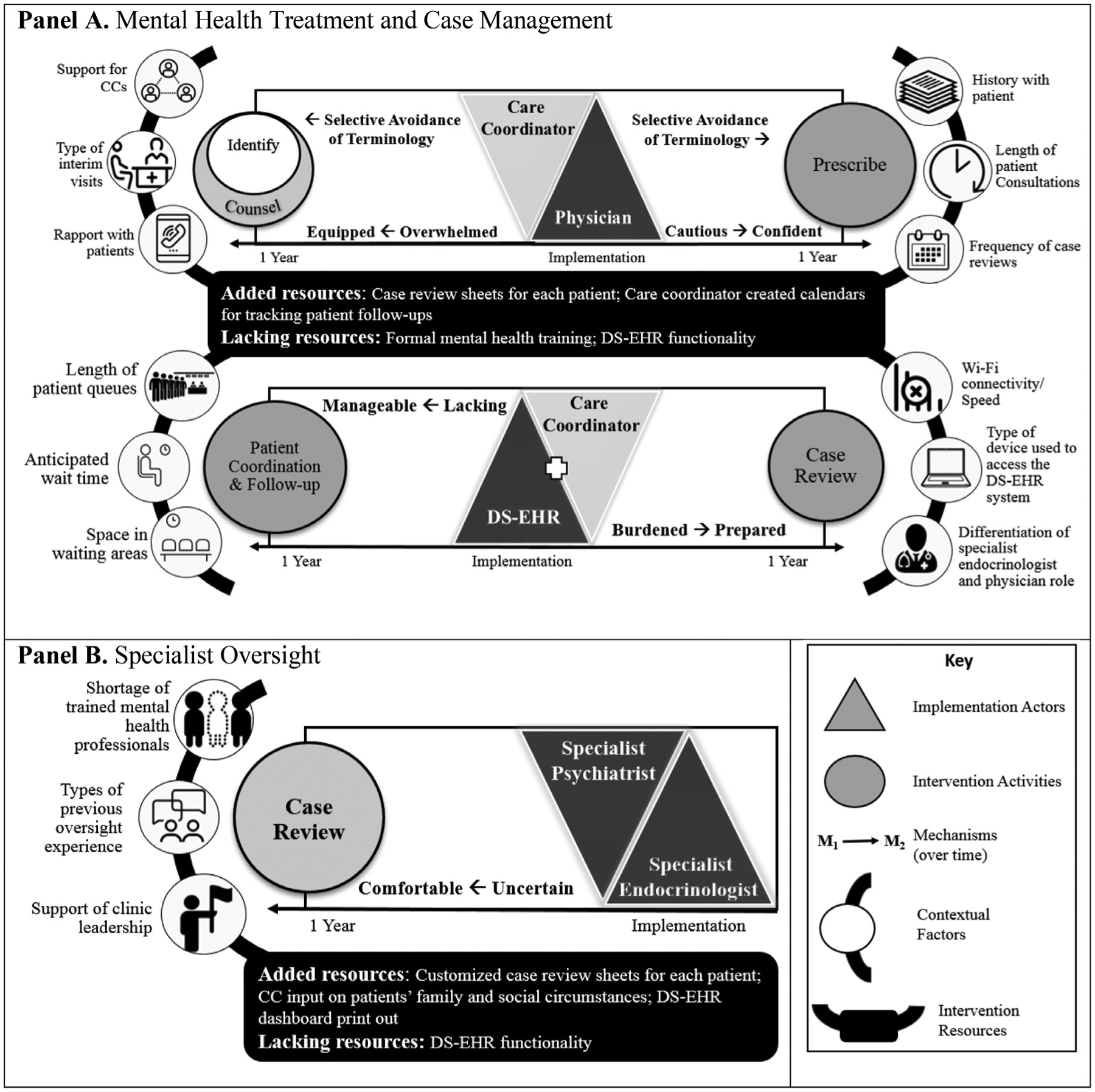
Efforts to enhance patient care coordination (i.e., adapting clinics’ patient flow and resources, on-going trainings, and on-site support for care coordinators) improved implementation of depression treatment by usual care diabetes physicians. Clinician's avoidance of the term depression was identified as a barrier to mental health counseling and treatment.
Conclusions
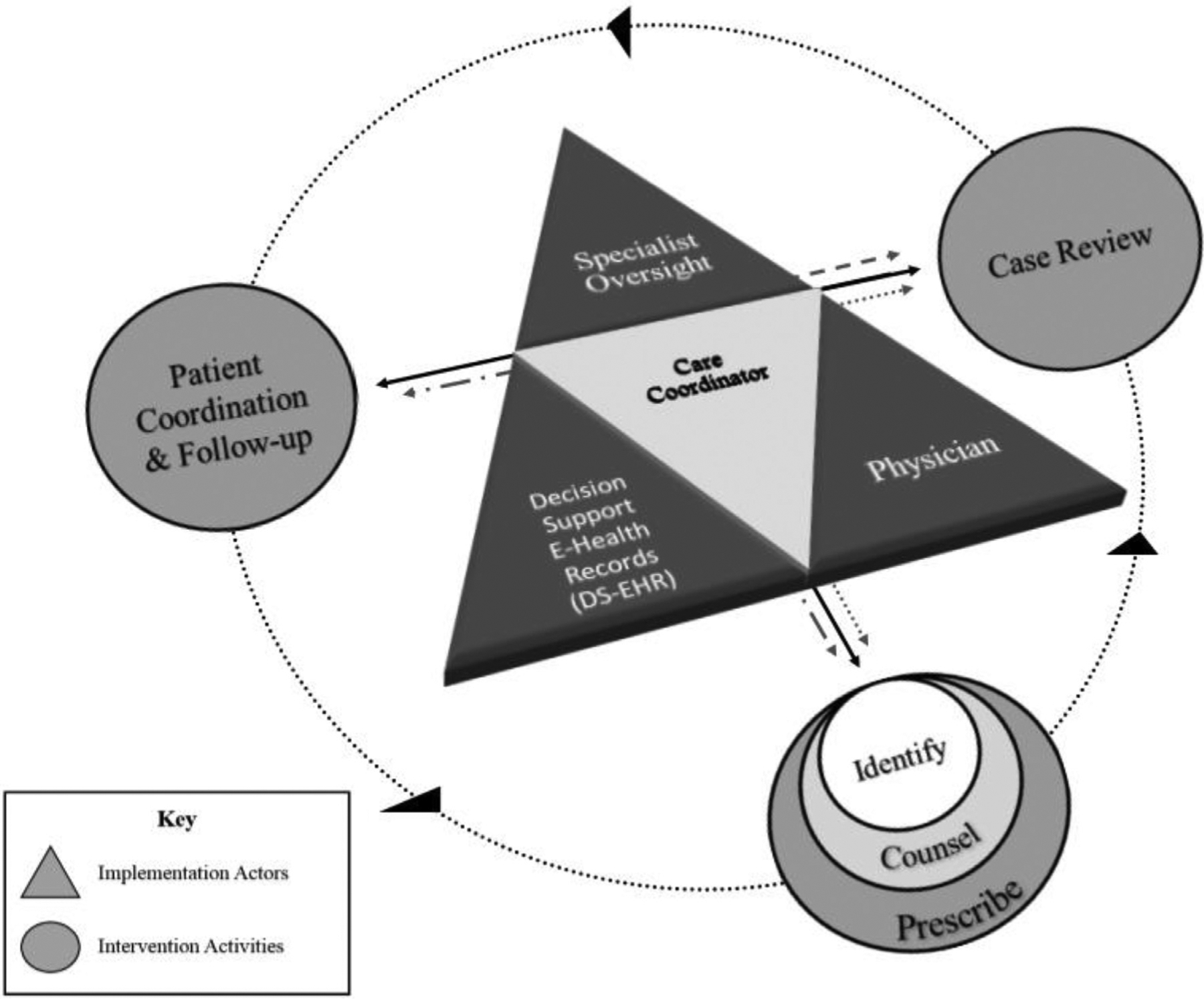
The variations in organizational features and processes linked to implementation activities across two clinics provided an opportunity to examine how and why different contextual factors help or hinder the implementation process. Findings from this study demonstrate that successful implementation of an integrated depression and diabetes care model is feasible in a low-resource setting, while the revised program theories provide an explanatory framework of coordinated care implementation processes that can inform future efforts to disseminate and scale this care model.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
