Sanu Rajendraprasad, Molly Wheeler, Erin Wieruszewski, Joseph Gottwald, Lindsey A Wallace, Danielle Gerberi, Patrick M Wieruszewski, Nathan J Smischney
{"title":"Clonidine use during dexmedetomidine weaning: A systematic review.","authors":"Sanu Rajendraprasad, Molly Wheeler, Erin Wieruszewski, Joseph Gottwald, Lindsey A Wallace, Danielle Gerberi, Patrick M Wieruszewski, Nathan J Smischney","doi":"10.5492/wjccm.v12.i1.18","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Dexmedetomidine is a centrally acting alpha-2A adrenergic agonist that is commonly used as a sedative and anxiolytic in the intensive care unit (ICU), with prolonged use increasing risk of withdrawal symptoms upon sudden discontinuation. As clonidine is an enterally available alpha-2A adrenergic agonist, it may be a suitable agent to taper off dexmedetomidine and reduce withdrawal syndromes. The appropriate dosing and conversion strategies for using enteral clonidine in this context are not known. The objective of this systematic review is to summarize the evidence of enteral clonidine application during dexmedetomidine weaning for prevention of withdrawal symptoms.</p><p><strong>Aim: </strong>To systematically review the practice, dosing schema, and outcomes of enteral clonidine use during dexmedetomidine weaning in critically ill adults.</p><p><strong>Methods: </strong>This was a systematic review of enteral clonidine used during dexmedetomidine weaning in critically ill adults (≥ 18 years). Randomized controlled trials, prospective cohorts, and retrospective cohorts evaluating the use of clonidine to wean patients from dexmedetomidine in the critically ill were included. The primary outcomes of interest were dosing and titration schema of enteral clonidine and dexmedetomidine and risk factors for dexmedetomidine withdrawal. Other secondary outcomes included prevalence of adverse events associated with enteral clonidine use, re-initiation of dexmedetomidine, duration of mechanical ventilation, and ICU length of stay.</p><p><strong>Results: </strong>A total of 3427 studies were screened for inclusion with three meeting inclusion criteria with a total of 88 patients. All three studies were observational, two being prospective and one retrospective. In all included studies, the choice to start enteral clonidine to wean off dexmedetomidine was made at the discretion of the physician. Weaning time ranged from 13 to 167 h on average. Enteral clonidine was started in the prospective studies in a similar protocolized method, with 0.3 mg every 6 h. After starting clonidine, patients remained on dexmedetomidine for a median of 1-28 h. Following the termination of dexmedetomidine, two trials tapered enteral clonidine by increasing the interval every 24 h from 6 h to 8h, 12h, and 24 h, followed by clonidine discontinuation. For indicators of enteral clonidine withdrawal, the previously tolerable dosage was reinstated for several days before resuming the taper on the same protocol. The adverse events associated with enteral clonidine use were higher than patients on dexmedetomidine taper alone with increased agitation. The re-initiation of dexmedetomidine was not documented in any study. Only 17 (37%) patients were mechanically ventilated with median duration of 3.5 d for 13 patients in one of the 2 studies. ICU lengths of stay were similar.</p><p><strong>Conclusion: </strong>Enteral clonidine is a strategy to wean critically ill patients from dexmedetomidine. There is an association of increased withdrawal symptoms and agitation with the use of a clonidine taper.</p>","PeriodicalId":66959,"journal":{"name":"世界危重病急救学杂志(英文版)","volume":"12 1","pages":"18-28"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/44/09/WJCCM-12-18.PMC9846870.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界危重病急救学杂志(英文版)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5492/wjccm.v12.i1.18","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Dexmedetomidine is a centrally acting alpha-2A adrenergic agonist that is commonly used as a sedative and anxiolytic in the intensive care unit (ICU), with prolonged use increasing risk of withdrawal symptoms upon sudden discontinuation. As clonidine is an enterally available alpha-2A adrenergic agonist, it may be a suitable agent to taper off dexmedetomidine and reduce withdrawal syndromes. The appropriate dosing and conversion strategies for using enteral clonidine in this context are not known. The objective of this systematic review is to summarize the evidence of enteral clonidine application during dexmedetomidine weaning for prevention of withdrawal symptoms.
Aim: To systematically review the practice, dosing schema, and outcomes of enteral clonidine use during dexmedetomidine weaning in critically ill adults.
Methods: This was a systematic review of enteral clonidine used during dexmedetomidine weaning in critically ill adults (≥ 18 years). Randomized controlled trials, prospective cohorts, and retrospective cohorts evaluating the use of clonidine to wean patients from dexmedetomidine in the critically ill were included. The primary outcomes of interest were dosing and titration schema of enteral clonidine and dexmedetomidine and risk factors for dexmedetomidine withdrawal. Other secondary outcomes included prevalence of adverse events associated with enteral clonidine use, re-initiation of dexmedetomidine, duration of mechanical ventilation, and ICU length of stay.
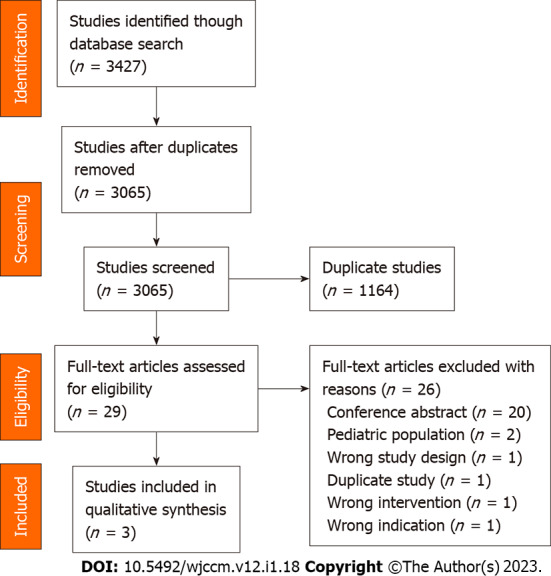
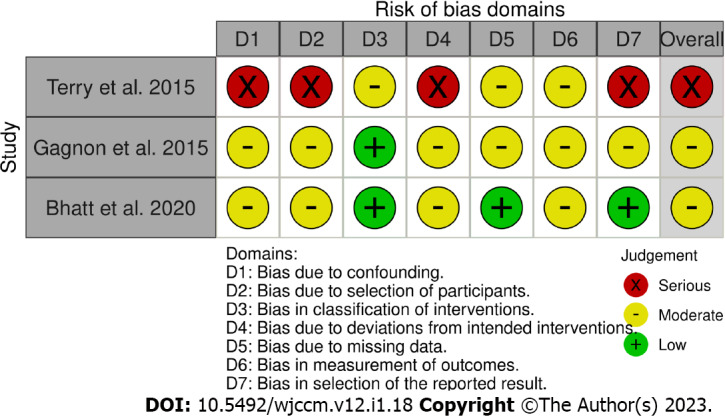
Results: A total of 3427 studies were screened for inclusion with three meeting inclusion criteria with a total of 88 patients. All three studies were observational, two being prospective and one retrospective. In all included studies, the choice to start enteral clonidine to wean off dexmedetomidine was made at the discretion of the physician. Weaning time ranged from 13 to 167 h on average. Enteral clonidine was started in the prospective studies in a similar protocolized method, with 0.3 mg every 6 h. After starting clonidine, patients remained on dexmedetomidine for a median of 1-28 h. Following the termination of dexmedetomidine, two trials tapered enteral clonidine by increasing the interval every 24 h from 6 h to 8h, 12h, and 24 h, followed by clonidine discontinuation. For indicators of enteral clonidine withdrawal, the previously tolerable dosage was reinstated for several days before resuming the taper on the same protocol. The adverse events associated with enteral clonidine use were higher than patients on dexmedetomidine taper alone with increased agitation. The re-initiation of dexmedetomidine was not documented in any study. Only 17 (37%) patients were mechanically ventilated with median duration of 3.5 d for 13 patients in one of the 2 studies. ICU lengths of stay were similar.
Conclusion: Enteral clonidine is a strategy to wean critically ill patients from dexmedetomidine. There is an association of increased withdrawal symptoms and agitation with the use of a clonidine taper.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
