Impact of pre-operative transjugular intrahepatic portosystemic shunt on post-operative outcomes following non-transplant surgeries in patients with decompensated cirrhosis.
Pragnesh Patel, Malcolm Irani, Edward A Graviss, Duc T Nguyen, Eamonn M M Quigley, David W Victor
{"title":"Impact of pre-operative transjugular intrahepatic portosystemic shunt on post-operative outcomes following non-transplant surgeries in patients with decompensated cirrhosis.","authors":"Pragnesh Patel, Malcolm Irani, Edward A Graviss, Duc T Nguyen, Eamonn M M Quigley, David W Victor","doi":"10.21037/tgh-21-133","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with cirrhosis have a high risk for morbidity and mortality in relation to abdominal surgery. Despite improvements in surgical techniques and intensive care, major abdominal surgery still remains a challenge. Major factors determining short- and long-term survival and perioperative complications in this patient population include severity of liver dysfunction, degree of portal hypertension (PHTN), and the presence of related complications such as ascites. Elective transjugular intrahepatic portosystemic shunt (TIPS) placement prior to surgery has been reported to improve perioperative outcomes, but available data is limited to case reports and small case series. We aimed to determine the impact of elective TIPS placement on perioperative outcomes after abdominal-pelvic surgeries in patients with cirrhosis.</p><p><strong>Methods: </strong>We performed a retrospective chart review of patients who underwent elective TIPS and compared these patients with a cohort of cirrhotic patients who underwent any abdominal surgeries without TIPS placement. The primary outcomes were mortality at 30 days and 1 year following surgery. Other post-operative outcomes compared between the two groups, included: blood loss, worsening ascites, wound leak, infections, encephalopathy, liver decompensation, and length of hospitalization.</p><p><strong>Results: </strong>Among 38 patients with cirrhosis who underwent abdominal surgery, 20 patients underwent pre-operative elective TIPS placement. Demographic characteristics of the two groups were comparable including age, gender, and body mass index (BMI). The median age was 62 years with a male predominance (62.5%). Both groups had similar etiologies of cirrhosis with hepatitis C virus (HCV) (34.2%) being most common. The most frequent indications for surgery were strangulated hernia (50%) in the TIPS group and acute cholecystitis (55.6%) in the non-TIPS group. Mean pre-TIPS hepato-venous portal gradient (HVPG) was 16.5 mmHg and mean post-TIPS HVPG was 7.0 mmHg. Mortality at 1 month was not statistically different between the groups (20% <i>vs.</i> 5.6%, respectively, P=0.19). The 1-year mortality was also not statistically different between the two groups (20% <i>vs.</i> 11.1%, P=0.36).</p><p><strong>Conclusions: </strong>We found no statistically significant difference in mortality or rate of post-operative complications between patients who received pre-operative TIPS and those who did not in our age-matched cohort.</p>","PeriodicalId":23267,"journal":{"name":"Translational gastroenterology and hepatology","volume":"8 ","pages":"9"},"PeriodicalIF":3.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5a/00/tgh-08-21-133.PMC9813646.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational gastroenterology and hepatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tgh-21-133","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients with cirrhosis have a high risk for morbidity and mortality in relation to abdominal surgery. Despite improvements in surgical techniques and intensive care, major abdominal surgery still remains a challenge. Major factors determining short- and long-term survival and perioperative complications in this patient population include severity of liver dysfunction, degree of portal hypertension (PHTN), and the presence of related complications such as ascites. Elective transjugular intrahepatic portosystemic shunt (TIPS) placement prior to surgery has been reported to improve perioperative outcomes, but available data is limited to case reports and small case series. We aimed to determine the impact of elective TIPS placement on perioperative outcomes after abdominal-pelvic surgeries in patients with cirrhosis.
Methods: We performed a retrospective chart review of patients who underwent elective TIPS and compared these patients with a cohort of cirrhotic patients who underwent any abdominal surgeries without TIPS placement. The primary outcomes were mortality at 30 days and 1 year following surgery. Other post-operative outcomes compared between the two groups, included: blood loss, worsening ascites, wound leak, infections, encephalopathy, liver decompensation, and length of hospitalization.
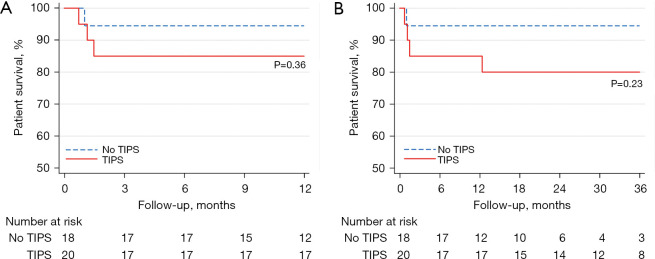
Results: Among 38 patients with cirrhosis who underwent abdominal surgery, 20 patients underwent pre-operative elective TIPS placement. Demographic characteristics of the two groups were comparable including age, gender, and body mass index (BMI). The median age was 62 years with a male predominance (62.5%). Both groups had similar etiologies of cirrhosis with hepatitis C virus (HCV) (34.2%) being most common. The most frequent indications for surgery were strangulated hernia (50%) in the TIPS group and acute cholecystitis (55.6%) in the non-TIPS group. Mean pre-TIPS hepato-venous portal gradient (HVPG) was 16.5 mmHg and mean post-TIPS HVPG was 7.0 mmHg. Mortality at 1 month was not statistically different between the groups (20% vs. 5.6%, respectively, P=0.19). The 1-year mortality was also not statistically different between the two groups (20% vs. 11.1%, P=0.36).
Conclusions: We found no statistically significant difference in mortality or rate of post-operative complications between patients who received pre-operative TIPS and those who did not in our age-matched cohort.
背景:肝硬化患者在腹部手术时有很高的发病率和死亡率。尽管外科技术和重症监护有所改进,腹部大手术仍然是一个挑战。决定该患者群体短期和长期生存及围手术期并发症的主要因素包括肝功能障碍的严重程度、门静脉高压程度(PHTN)以及相关并发症如腹水的存在。择期经颈静脉肝内门系统分流术(TIPS)可改善围手术期预后,但现有数据仅限于病例报告和小病例系列。我们的目的是确定选择性TIPS放置对肝硬化患者腹盆腔手术后围手术期结局的影响。方法:我们对接受选择性TIPS的患者进行了回顾性图表回顾,并将这些患者与接受任何腹部手术但未放置TIPS的肝硬化患者进行了比较。主要结局是术后30天和1年的死亡率。两组之间比较的其他术后结果包括:失血、腹水恶化、伤口渗漏、感染、脑病、肝功能失代偿和住院时间。结果:38例接受腹部手术的肝硬化患者中,20例患者术前择期置放TIPS。两组的人口统计学特征具有可比性,包括年龄、性别和身体质量指数(BMI)。中位年龄62岁,男性居多(62.5%)。两组肝硬化病因相似,以丙型肝炎病毒(HCV)最常见(34.2%)。TIPS组最常见的手术指征是绞窄性疝(50%),非TIPS组急性胆囊炎(55.6%)。tips前平均肝静脉门静脉梯度(HVPG)为16.5 mmHg, tips后平均HVPG为7.0 mmHg。组间1个月死亡率无统计学差异(分别为20% vs. 5.6%, P=0.19)。两组的1年死亡率也无统计学差异(20% vs. 11.1%, P=0.36)。结论:我们发现,在年龄匹配的队列中,术前接受TIPS治疗的患者和未接受TIPS治疗的患者在死亡率和术后并发症发生率方面没有统计学上的显著差异。
期刊介绍:
Translational Gastroenterology and Hepatology (Transl Gastroenterol Hepatol; TGH; Online ISSN 2415-1289) is an open-access, peer-reviewed online journal that focuses on cutting-edge findings in the field of translational research in gastroenterology and hepatology and provides current and practical information on diagnosis, prevention and clinical investigations of gastrointestinal, pancreas, gallbladder and hepatic diseases. Specific areas of interest include, but not limited to, multimodality therapy, biomarkers, imaging, biology, pathology, and technical advances related to gastrointestinal and hepatic diseases. Contributions pertinent to gastroenterology and hepatology are also included from related fields such as nutrition, surgery, public health, human genetics, basic sciences, education, sociology, and nursing.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
