Ryuichiro Yagi, Shinichi Goto, Yoshinori Katsumata, Calum A MacRae, Rahul C Deo
{"title":"Importance of external validation and subgroup analysis of artificial intelligence in the detection of low ejection fraction from electrocardiograms.","authors":"Ryuichiro Yagi, Shinichi Goto, Yoshinori Katsumata, Calum A MacRae, Rahul C Deo","doi":"10.1093/ehjdh/ztac065","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>Left ventricular systolic dysfunction (LVSD) carries an increased risk for overt heart failure and mortality, yet treatable to mitigate disease progression. An artificial intelligence (AI)-enabled 12-lead electrocardiogram (ECG) model demonstrated promise in LVSD screening, but the performance dropped unexpectedly in external validation. We thus sought to train <i>de novo</i> models for LVSD detection and investigated their performance across multiple institutions and across a broader set of patient strata.</p><p><strong>Methods and results: </strong>ECGs taken within 14 days of an echocardiogram were obtained from four academic hospitals (three in the United States and one in Japan). Four AI models were trained to detect patients with ejection fraction (EF) <40% using ECGs from each of the four institutions. All the models were then evaluated on the held-out test data set from the same institution and data from the three external institutions. Subgroup analyses stratified by patient characteristics and common ECG abnormalities were performed. A total of 221 846 ECGs were identified from the 4 institutions. While the Brigham and Women's Hospital (BWH)-trained and Keio-trained models yielded similar accuracy on their internal test data [area under the receiver operating curve (AUROC) 0.913 and 0.914, respectively], external validity was worse for the Keio-trained model (AUROC: 0.905-0.915 for BWH trained and 0.849-0.877 for Keio-trained model). Although ECG abnormalities including atrial fibrillation, left bundle branch block, and paced rhythm-reduced detection, the models performed robustly across patient characteristics and other ECG features.</p><p><strong>Conclusion: </strong>While using the same model architecture, different data sets produced models with different performances for detecting low-EF highlighting the importance of external validation and extensive stratification analysis.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"3 4","pages":"654-657"},"PeriodicalIF":4.4000,"publicationDate":"2022-11-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3c/b5/ztac065.PMC9779862.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztac065","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/12/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: Left ventricular systolic dysfunction (LVSD) carries an increased risk for overt heart failure and mortality, yet treatable to mitigate disease progression. An artificial intelligence (AI)-enabled 12-lead electrocardiogram (ECG) model demonstrated promise in LVSD screening, but the performance dropped unexpectedly in external validation. We thus sought to train de novo models for LVSD detection and investigated their performance across multiple institutions and across a broader set of patient strata.
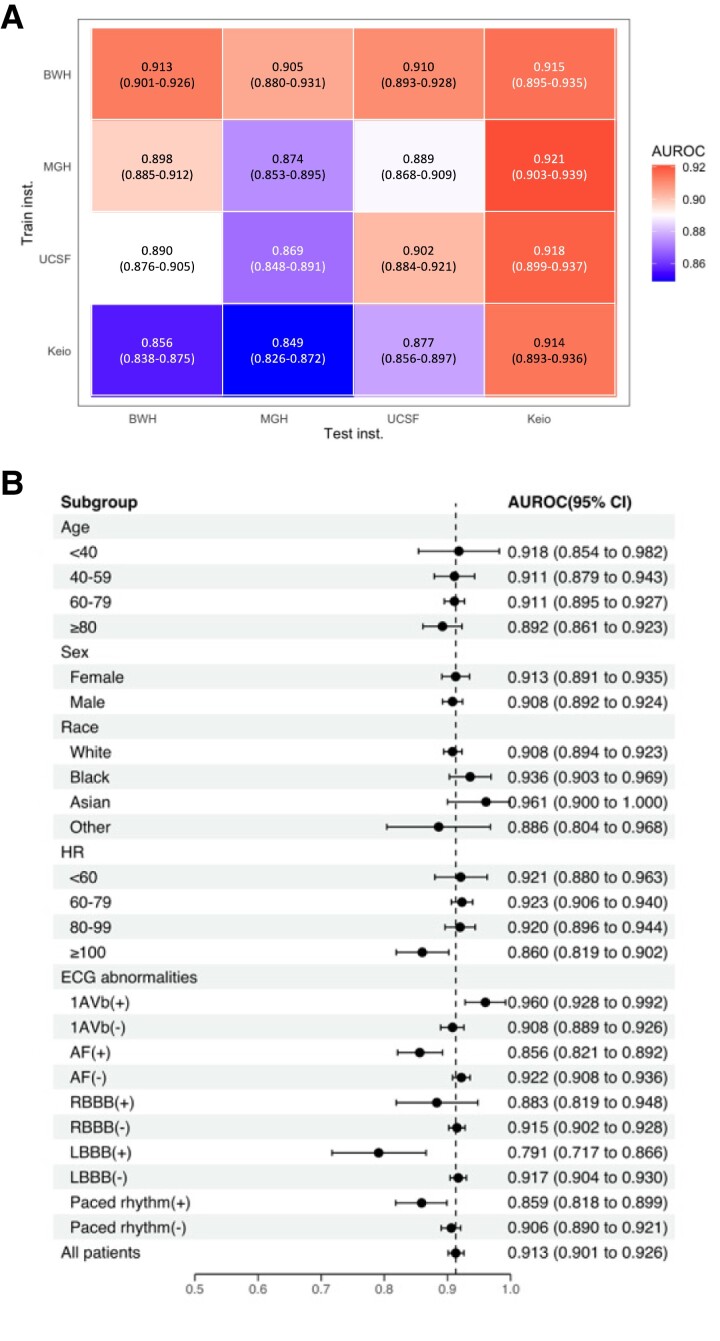
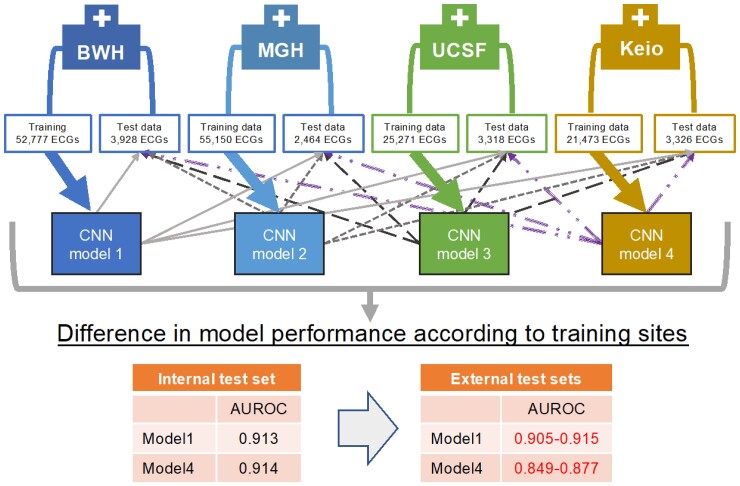
Methods and results: ECGs taken within 14 days of an echocardiogram were obtained from four academic hospitals (three in the United States and one in Japan). Four AI models were trained to detect patients with ejection fraction (EF) <40% using ECGs from each of the four institutions. All the models were then evaluated on the held-out test data set from the same institution and data from the three external institutions. Subgroup analyses stratified by patient characteristics and common ECG abnormalities were performed. A total of 221 846 ECGs were identified from the 4 institutions. While the Brigham and Women's Hospital (BWH)-trained and Keio-trained models yielded similar accuracy on their internal test data [area under the receiver operating curve (AUROC) 0.913 and 0.914, respectively], external validity was worse for the Keio-trained model (AUROC: 0.905-0.915 for BWH trained and 0.849-0.877 for Keio-trained model). Although ECG abnormalities including atrial fibrillation, left bundle branch block, and paced rhythm-reduced detection, the models performed robustly across patient characteristics and other ECG features.
Conclusion: While using the same model architecture, different data sets produced models with different performances for detecting low-EF highlighting the importance of external validation and extensive stratification analysis.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
