Andrea D Gloor, Gerald J Berry, Jorg J Goronzy, Cornelia M Weyand
{"title":"Age as a risk factor in vasculitis.","authors":"Andrea D Gloor, Gerald J Berry, Jorg J Goronzy, Cornelia M Weyand","doi":"10.1007/s00281-022-00911-1","DOIUrl":null,"url":null,"abstract":"<p><p>Two vasculitides, giant cell arteritis (GCA) and Takayasu arteritis (TAK), are recognized as autoimmune and autoinflammatory diseases that manifest exclusively within the aorta and its large branches. In both entities, the age of the affected host is a critical risk factor. TAK manifests during the 2nd-4th decade of life, occurring while the immune system is at its height of performance. GCA is a disease of older individuals, with infrequent cases during the 6th decade and peak incidence during the 8th decade of life. In both vasculitides, macrophages and T cells infiltrate into the adventitia and media of affected vessels, induce granulomatous inflammation, cause vessel wall destruction, and reprogram vascular cells to drive adventitial and neointimal expansion. In GCA, abnormal immunity originates in an aged immune system and evolves within the aged vascular microenvironment. One hallmark of the aging immune system is the preferential loss of CD8<sup>+</sup> T cell function. Accordingly, in GCA but not in TAK, CD8<sup>+</sup> effector T cells play a negligible role and anti-inflammatory CD8<sup>+</sup> T regulatory cells are selectively impaired. Here, we review current evidence of how the process of immunosenescence impacts the risk for GCA and how fundamental differences in the age of the immune system translate into differences in the granulomatous immunopathology of TAK versus GCA.</p>","PeriodicalId":21704,"journal":{"name":"Seminars in Immunopathology","volume":"44 3","pages":"281-301"},"PeriodicalIF":9.2000,"publicationDate":"2022-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9064861/pdf/","citationCount":"18","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Immunopathology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00281-022-00911-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 18
Abstract
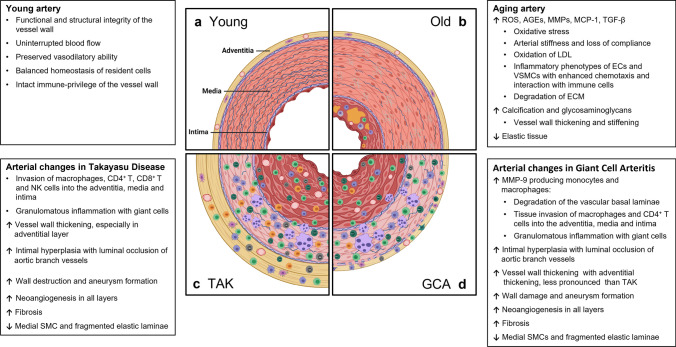
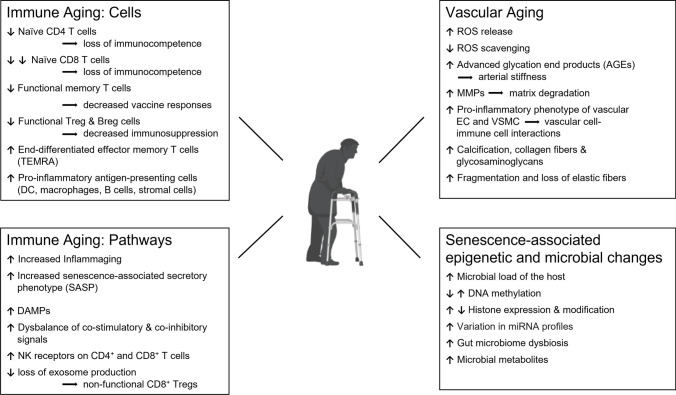
Two vasculitides, giant cell arteritis (GCA) and Takayasu arteritis (TAK), are recognized as autoimmune and autoinflammatory diseases that manifest exclusively within the aorta and its large branches. In both entities, the age of the affected host is a critical risk factor. TAK manifests during the 2nd-4th decade of life, occurring while the immune system is at its height of performance. GCA is a disease of older individuals, with infrequent cases during the 6th decade and peak incidence during the 8th decade of life. In both vasculitides, macrophages and T cells infiltrate into the adventitia and media of affected vessels, induce granulomatous inflammation, cause vessel wall destruction, and reprogram vascular cells to drive adventitial and neointimal expansion. In GCA, abnormal immunity originates in an aged immune system and evolves within the aged vascular microenvironment. One hallmark of the aging immune system is the preferential loss of CD8+ T cell function. Accordingly, in GCA but not in TAK, CD8+ effector T cells play a negligible role and anti-inflammatory CD8+ T regulatory cells are selectively impaired. Here, we review current evidence of how the process of immunosenescence impacts the risk for GCA and how fundamental differences in the age of the immune system translate into differences in the granulomatous immunopathology of TAK versus GCA.
期刊介绍:
The aim of Seminars in Immunopathology is to bring clinicians and pathologists up-to-date on developments in the field of immunopathology.For this purpose topical issues will be organized usually with the help of a guest editor.Recent developments are summarized in review articles by authors who have personally contributed to the specific topic.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
