Sujoy Khan, Charu Chopra, Alaistair Mitchell, Alla Nakonechna, Patrick Yong, Mohammed Yousuf Karim
{"title":"Resistant Chronic Spontaneous Urticaria - A Case Series Narrative Review of Treatment Options.","authors":"Sujoy Khan, Charu Chopra, Alaistair Mitchell, Alla Nakonechna, Patrick Yong, Mohammed Yousuf Karim","doi":"10.1177/21526575221144951","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic spontaneous urticaria (CSU) can be extremely debilitating to the patient and challenging for the treating clinician. The National Institute of Health and Clinical Excellence (NICE) in the United Kingdom (UK) recommendation of omalizumab for patients who fail to respond to high-dose anti-histamines has improved treatment options and quality of life. However, there is still lack of clear guidelines for treatment of patients resistant to standard and anti-IgE therapies.</p><p><strong>Methods: </strong>We discuss the therapeutic strategies employed among nine extremely resistant CSU cases and the heterogeneity between guidelines from different societies.</p><p><strong>Results: </strong>Patients with anti-histamine-resistant urticaria either remained on omalizumab or started on immunosuppressive drugs (dapsone or ciclosporin) when they stopped responding to omalizumab. We used clinical assessment, skin biopsies (when available) and previous published reports to consider dapsone (for predominantly neutrophilic infiltration), or ciclosporin at doses between 2 and 4 mg/kg/day. One patient with ciclosporin-resistant urticaria responded to mycophenolate mofetil. Two patients remain on long-term omalizumab due to its relative safety and efficacy including 1 patient with underlying antibody deficiency where omalizumab was preferred over risks of using immunosuppressive medications.</p><p><strong>Conclusions: </strong>These case studies bring to light the real-world difficulties in managing patients with resistant CSU and the need for generating the evidence base on alternative therapeutic options such as synergistic use of biologics and immunosuppressive drugs.</p>","PeriodicalId":45192,"journal":{"name":"Allergy & Rhinology","volume":"13 ","pages":"21526575221144951"},"PeriodicalIF":1.2000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d9/53/10.1177_21526575221144951.PMC9791268.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Allergy & Rhinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/21526575221144951","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 2
Abstract
Background: Chronic spontaneous urticaria (CSU) can be extremely debilitating to the patient and challenging for the treating clinician. The National Institute of Health and Clinical Excellence (NICE) in the United Kingdom (UK) recommendation of omalizumab for patients who fail to respond to high-dose anti-histamines has improved treatment options and quality of life. However, there is still lack of clear guidelines for treatment of patients resistant to standard and anti-IgE therapies.
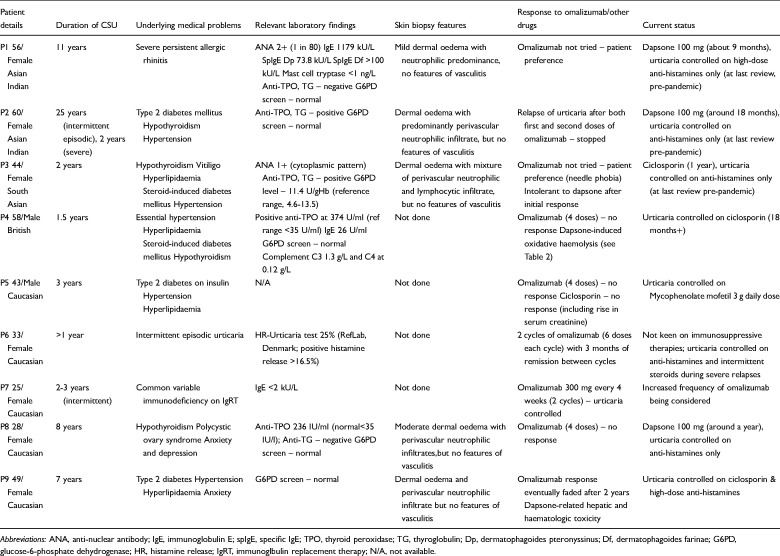
Methods: We discuss the therapeutic strategies employed among nine extremely resistant CSU cases and the heterogeneity between guidelines from different societies.
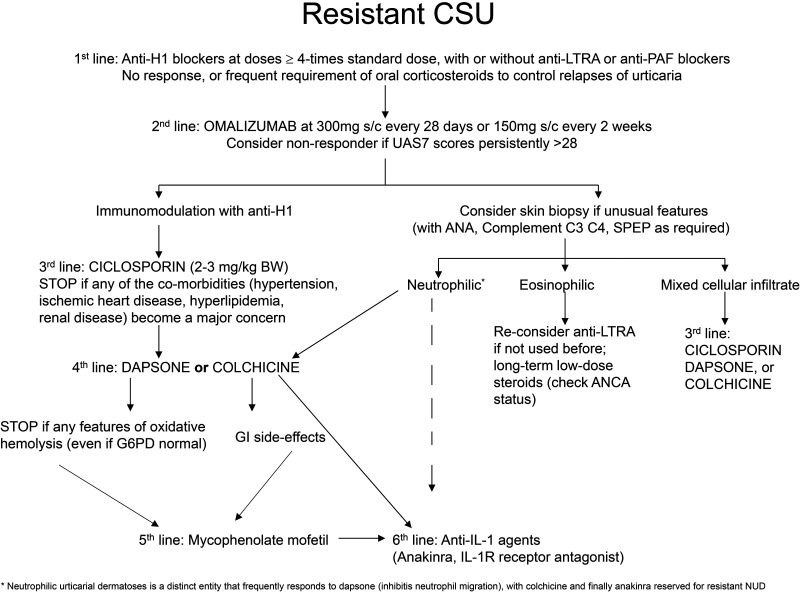
Results: Patients with anti-histamine-resistant urticaria either remained on omalizumab or started on immunosuppressive drugs (dapsone or ciclosporin) when they stopped responding to omalizumab. We used clinical assessment, skin biopsies (when available) and previous published reports to consider dapsone (for predominantly neutrophilic infiltration), or ciclosporin at doses between 2 and 4 mg/kg/day. One patient with ciclosporin-resistant urticaria responded to mycophenolate mofetil. Two patients remain on long-term omalizumab due to its relative safety and efficacy including 1 patient with underlying antibody deficiency where omalizumab was preferred over risks of using immunosuppressive medications.
Conclusions: These case studies bring to light the real-world difficulties in managing patients with resistant CSU and the need for generating the evidence base on alternative therapeutic options such as synergistic use of biologics and immunosuppressive drugs.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
