Israel Agaku, Caleb Adeoye, Naa Adjeley Anamor Krow, Theodore Long
{"title":"Segmentation analysis of the unvaccinated US adult population 2 years into the COVID-19 pandemic, 1 December 2021 to 7 February 2022.","authors":"Israel Agaku, Caleb Adeoye, Naa Adjeley Anamor Krow, Theodore Long","doi":"10.1136/fmch-2022-001769","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>We performed a segmentation analysis of the unvaccinated adult US population to identify sociodemographic and psychographic characteristics of those who were vaccine accepting, vaccine unsure and vaccine averse.</p><p><strong>Design: </strong>Cross-sectional.</p><p><strong>Setting: </strong>Nationally representative, web-based survey.</p><p><strong>Participants: </strong>211 303 participants aged ≥18 years were asked in the Household Pulse Survey conducted during 1 December 2021 to 7 February 2022, whether they had ever received a COVID-19 vaccine. Those answering 'No' were asked their receptivity to the vaccine and their responses were categorised as vaccine averse, unsure and accepting. Adjusted prevalence ratios (APR) were calculated in separate multivariable Poisson regression models to evaluate the correlation of the three vaccine dispositions.</p><p><strong>Results: </strong>Overall, 15.2% of US adults were unvaccinated during 1 December 2021 to 7 February 2022, ranging from 5.8% in District of Columbia to 29.0% in Wyoming. Of the entire unvaccinated population nationwide, 51.0% were vaccine averse, 35.0% vaccine unsure and 14.0% vaccine accepting. The likelihood of vaccine aversion was higher among those self-employed (APR=1.11, 95% CI 1.02 to 1.22) or working in a private company (APR=1.09, 95% CI 1.01 to 1.17) than those unemployed; living in a detached, single-family house than in a multiunit apartment (APR=1.15, 95% CI 1.04 to 1.26); and insured by Veterans Affairs/Tricare than uninsured (APR=1.22, 95% CI 1.01 to 1.47). Reasons for having not yet received a vaccine differed among those vaccine accepting, unsure and averse. The percentage reporting logistical or access-related barriers to getting a vaccine (eg, difficulty getting a vaccine, or perceived cost of the vaccine) was relatively higher than those vaccine accepting. Those vaccine unsure reported the highest prevalence of barriers related to perceived safety/effectiveness, including wanting to 'wait and see' if the vaccines were safe (45.2%) and uncertainty whether the vaccines would be effective in protecting them from COVID-19 (29.6%). Those vaccine averse reported the highest prevalence for barriers pertaining to lack of trust in the government or in the vaccines (50.1% and 57.5% respectively), the perception that COVID-19 was not that big of a threat (32.2%) and the perception that they did not need a vaccine (42.3%).</p><p><strong>Conclusions: </strong>The unvaccinated segment of the population is not a monolith, and a substantial segment may still get vaccinated if constraining factors are adequately addressed.</p>","PeriodicalId":44590,"journal":{"name":"Family Medicine and Community Health","volume":"11 1","pages":""},"PeriodicalIF":4.3000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/32/42/fmch-2022-001769.PMC9943697.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Family Medicine and Community Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/fmch-2022-001769","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: We performed a segmentation analysis of the unvaccinated adult US population to identify sociodemographic and psychographic characteristics of those who were vaccine accepting, vaccine unsure and vaccine averse.
Participants: 211 303 participants aged ≥18 years were asked in the Household Pulse Survey conducted during 1 December 2021 to 7 February 2022, whether they had ever received a COVID-19 vaccine. Those answering 'No' were asked their receptivity to the vaccine and their responses were categorised as vaccine averse, unsure and accepting. Adjusted prevalence ratios (APR) were calculated in separate multivariable Poisson regression models to evaluate the correlation of the three vaccine dispositions.
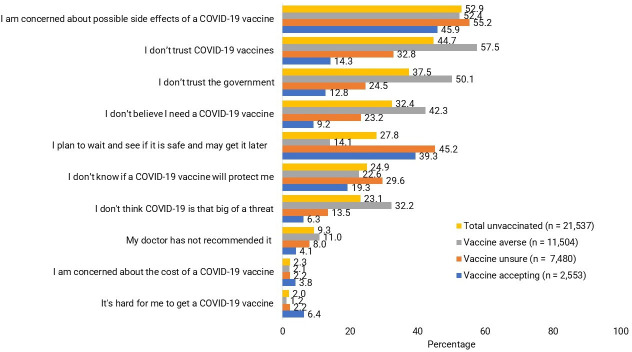
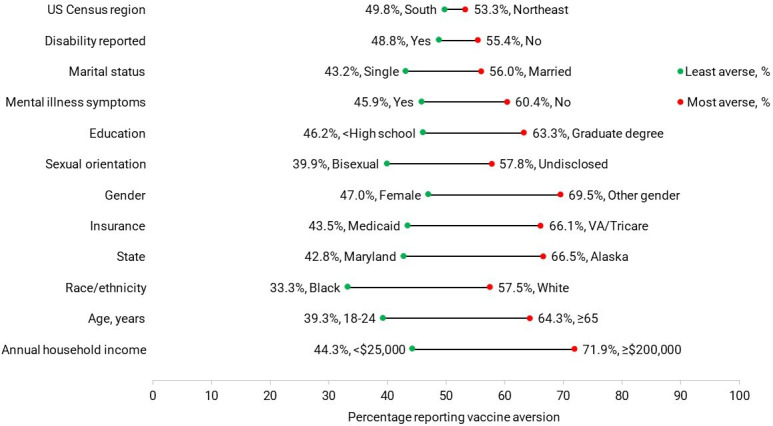
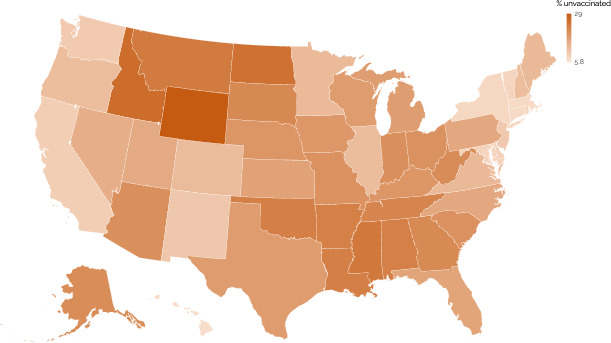
Results: Overall, 15.2% of US adults were unvaccinated during 1 December 2021 to 7 February 2022, ranging from 5.8% in District of Columbia to 29.0% in Wyoming. Of the entire unvaccinated population nationwide, 51.0% were vaccine averse, 35.0% vaccine unsure and 14.0% vaccine accepting. The likelihood of vaccine aversion was higher among those self-employed (APR=1.11, 95% CI 1.02 to 1.22) or working in a private company (APR=1.09, 95% CI 1.01 to 1.17) than those unemployed; living in a detached, single-family house than in a multiunit apartment (APR=1.15, 95% CI 1.04 to 1.26); and insured by Veterans Affairs/Tricare than uninsured (APR=1.22, 95% CI 1.01 to 1.47). Reasons for having not yet received a vaccine differed among those vaccine accepting, unsure and averse. The percentage reporting logistical or access-related barriers to getting a vaccine (eg, difficulty getting a vaccine, or perceived cost of the vaccine) was relatively higher than those vaccine accepting. Those vaccine unsure reported the highest prevalence of barriers related to perceived safety/effectiveness, including wanting to 'wait and see' if the vaccines were safe (45.2%) and uncertainty whether the vaccines would be effective in protecting them from COVID-19 (29.6%). Those vaccine averse reported the highest prevalence for barriers pertaining to lack of trust in the government or in the vaccines (50.1% and 57.5% respectively), the perception that COVID-19 was not that big of a threat (32.2%) and the perception that they did not need a vaccine (42.3%).
Conclusions: The unvaccinated segment of the population is not a monolith, and a substantial segment may still get vaccinated if constraining factors are adequately addressed.
目的:我们对未接种疫苗的美国成年人群进行了分割分析,以确定接受疫苗、不确定疫苗和厌恶疫苗人群的社会人口学和心理特征。设计:横断面。背景:具有全国代表性的网络调查。参与者:在2021年12月1日至2022年2月7日进行的家庭脉搏调查中,211 303名年龄≥18岁的参与者被问及是否曾接种过COVID-19疫苗。回答“否”的人被问及他们对疫苗的接受程度,他们的回答被归类为疫苗厌恶,不确定和接受。在单独的多变量泊松回归模型中计算校正患病率(APR),以评估三种疫苗配置的相关性。总体而言,在2021年12月1日至2022年2月7日期间,15.2%的美国成年人未接种疫苗,从哥伦比亚特区的5.8%到怀俄明州的29.0%不等。在全国未接种疫苗的人口中,51.0%的人反对疫苗,35.0%的人不确定疫苗,14.0%的人接受疫苗。个体经营者(APR=1.11, 95% CI 1.02至1.22)或私营企业工作者(APR=1.09, 95% CI 1.01至1.17)厌恶疫苗的可能性高于失业者;住在独立的单户住宅比住在多单元公寓(APR=1.15, 95% CI 1.04至1.26);有退伍军人事务部/Tricare保险的人比没有保险的人多(APR=1.22, 95% CI 1.01至1.47)。在接受疫苗、不确定疫苗和反对疫苗的人群中,尚未接种疫苗的原因有所不同。报告在获得疫苗方面存在后勤或获取相关障碍(例如,获得疫苗的困难或疫苗的感知成本)的百分比相对高于接受疫苗的百分比。那些不确定疫苗的人报告说,与感知安全性/有效性相关的障碍患病率最高,包括想要“等着看”疫苗是否安全(45.2%),以及不确定疫苗是否能有效保护他们免受COVID-19的侵害(29.6%)。那些反对疫苗的人报告说,对政府或疫苗缺乏信任(分别为50.1%和57.5%)、认为新冠病毒的威胁没有那么大(32.2%)、认为自己不需要疫苗(42.3%)等障碍的患病率最高。结论:未接种人群不是一个整体,如果限制因素得到充分解决,仍有相当一部分人可能接种疫苗。
期刊介绍:
Family Medicine and Community Health (FMCH) is a peer-reviewed, open-access journal focusing on the topics of family medicine, general practice and community health. FMCH strives to be a leading international journal that promotes ‘Health Care for All’ through disseminating novel knowledge and best practices in primary care, family medicine, and community health. FMCH publishes original research, review, methodology, commentary, reflection, and case-study from the lens of population health. FMCH’s Asian Focus section features reports of family medicine development in the Asia-pacific region. FMCH aims to be an exemplary forum for the timely communication of medical knowledge and skills with the goal of promoting improved health care through the practice of family and community-based medicine globally. FMCH aims to serve a diverse audience including researchers, educators, policymakers and leaders of family medicine and community health. We also aim to provide content relevant for researchers working on population health, epidemiology, public policy, disease control and management, preventative medicine and disease burden. FMCH does not impose any article processing charges (APC) or submission charges.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
