Hasan M Al-Dorzi, Haifa Al Mejedea, Reema Nazer, Yara Alhusaini, Aminah Alhamdan, Ajyad Al Jawad
{"title":"Occurrence, Risk Factors, and Outcomes of Pulmonary Barotrauma in Critically Ill COVID-19 Patients: A Retrospective Cohort Study.","authors":"Hasan M Al-Dorzi, Haifa Al Mejedea, Reema Nazer, Yara Alhusaini, Aminah Alhamdan, Ajyad Al Jawad","doi":"10.1155/2023/4675910","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Pulmonary barotrauma has been frequently observed in patients with COVID-19 who present with acute hypoxemic respiratory failure. This study evaluated the prevalence, risk factors, and outcomes of barotrauma in patients with COVID-19 requiring ICU admission.</p><p><strong>Methods: </strong>This retrospective cohort study included patients with confirmed COVID-19 who were admitted to an adult ICU between March and December 2020. We compared patients who had barotrauma with those who did not. A multivariable logistic regression analysis was performed to determine the predictors of barotrauma and hospital mortality.</p><p><strong>Results: </strong>Of 481 patients in the study cohort, 49 (10.2%, 95% confidence interval: 7.6-13.2%) developed barotrauma on a median of 4 days after ICU admission. Barotrauma manifested as pneumothorax (<i>N</i> = 21), pneumomediastinum (<i>N</i> = 25), and subcutaneous emphysema (<i>N</i> = 25) with frequent overlap. Chronic comorbidities and inflammatory markers were similar in both patient groups. Barotrauma occurred in 4/132 patients (3.0%) who received noninvasive ventilation without intubation, and in 43/280 patients (15.4%) who received invasive mechanical ventilation. Invasive mechanical ventilation was the only risk factor for barotrauma (odds ratio: 14.558, 95% confidence interval: 1.833-115.601). Patients with barotrauma had higher hospital mortality (69.4% versus 37.0%; <i>p</i> < 0.0001) and longer duration of mechanical ventilation and ICU stay. Barotrauma was an independent predictor of hospital mortality (odds ratio: 2.784, 95% confidence interval: 1.310-5.918).</p><p><strong>Conclusion: </strong>s. Barotrauma was common in critical COVID-19, with invasive mechanical ventilation being the most prominent risk factor. Barotrauma was associated with poorer clinical outcomes and was an independent predictor of hospital mortality.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2023 ","pages":"4675910"},"PeriodicalIF":1.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9977517/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/4675910","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 1
Abstract
Objective: Pulmonary barotrauma has been frequently observed in patients with COVID-19 who present with acute hypoxemic respiratory failure. This study evaluated the prevalence, risk factors, and outcomes of barotrauma in patients with COVID-19 requiring ICU admission.
Methods: This retrospective cohort study included patients with confirmed COVID-19 who were admitted to an adult ICU between March and December 2020. We compared patients who had barotrauma with those who did not. A multivariable logistic regression analysis was performed to determine the predictors of barotrauma and hospital mortality.
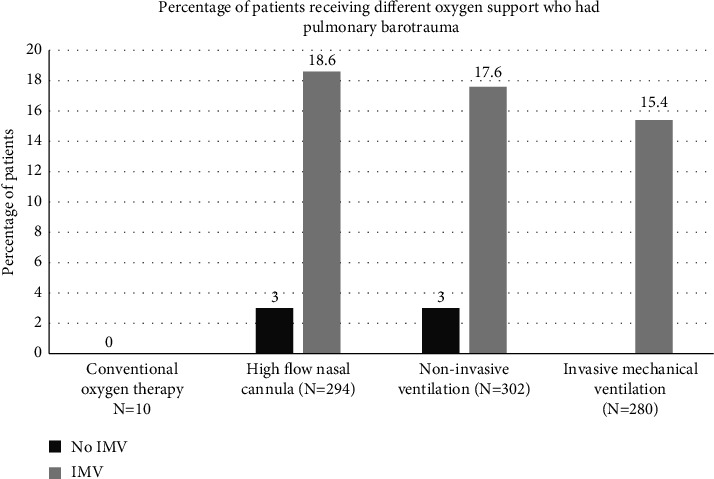
Results: Of 481 patients in the study cohort, 49 (10.2%, 95% confidence interval: 7.6-13.2%) developed barotrauma on a median of 4 days after ICU admission. Barotrauma manifested as pneumothorax (N = 21), pneumomediastinum (N = 25), and subcutaneous emphysema (N = 25) with frequent overlap. Chronic comorbidities and inflammatory markers were similar in both patient groups. Barotrauma occurred in 4/132 patients (3.0%) who received noninvasive ventilation without intubation, and in 43/280 patients (15.4%) who received invasive mechanical ventilation. Invasive mechanical ventilation was the only risk factor for barotrauma (odds ratio: 14.558, 95% confidence interval: 1.833-115.601). Patients with barotrauma had higher hospital mortality (69.4% versus 37.0%; p < 0.0001) and longer duration of mechanical ventilation and ICU stay. Barotrauma was an independent predictor of hospital mortality (odds ratio: 2.784, 95% confidence interval: 1.310-5.918).
Conclusion: s. Barotrauma was common in critical COVID-19, with invasive mechanical ventilation being the most prominent risk factor. Barotrauma was associated with poorer clinical outcomes and was an independent predictor of hospital mortality.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
