Analysis of Opioid Poisoning in Medically Underserved Rural Areas: An Evaluation of International Statistical Classification of Diseases Codes from the State of South Dakota.
{"title":"Analysis of Opioid Poisoning in Medically Underserved Rural Areas: An Evaluation of International Statistical Classification of Diseases Codes from the State of South Dakota.","authors":"Ahmed Nahian, Jewel Goodman Shepherd","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rural hospitals and patient population tend to be medically underserved. The states with more rural population dispensed the most opioids per person in the last 10 years. We aimed to explore if rurality contributed to the likelihood of higher opioid adversity and how it affected substance-use rehabilitation in federally designated Medically Underserved Areas (MUAs).</p><p><strong>Methods: </strong>We analyzed data dispensed by the South Dakota Department of Health (DOH) on opioid-led poisoning International Classification of Disease (ICD) codes that were active within the state in the last decade. After locating MUA rural and partially rural counties, we cross profiled the counties to the state datasets. Assessments were conducted using the PROC SURVEY methods in SAS version 9.3 (SAS Institute) and checked for multicollinearity with the Belsley-Kuh-Welsch technique. Finally, we used the American Hospital Association (AHA) database for analyzing substance use rehabilitation availability on per hospital basis.</p><p><strong>Results: </strong>The chi-square statistic for comparing opioid codes against non-opioid codes distributed among three categories, rural, non-rural, and partially rural was significant at the limit of p <0.05. 81.134% of opioid-led poisoning codes were activated in a rural county. Only four hospitals had substance-use rehabilitation, three of which were in a non-rural area. More people from the teenage and early-adulthood years (10-19) were prone to opioid usage.</p><p><strong>Conclusions: </strong>Rural counties in South Dakota were more likely to dispense opioid care and not have access to rehabilitation. We also found that as the opioid dispensing rate at hospitals within a state decreased as the state had less rural counties. Introducing public programs to train more physicians and cutting down cost of non-opioid based care may lower opioid distribution and increase rehabilitation options in rural hospitals.</p>","PeriodicalId":73583,"journal":{"name":"Journal of addiction research & therapy","volume":"13 11","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9974105/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of addiction research & therapy","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Rural hospitals and patient population tend to be medically underserved. The states with more rural population dispensed the most opioids per person in the last 10 years. We aimed to explore if rurality contributed to the likelihood of higher opioid adversity and how it affected substance-use rehabilitation in federally designated Medically Underserved Areas (MUAs).
Methods: We analyzed data dispensed by the South Dakota Department of Health (DOH) on opioid-led poisoning International Classification of Disease (ICD) codes that were active within the state in the last decade. After locating MUA rural and partially rural counties, we cross profiled the counties to the state datasets. Assessments were conducted using the PROC SURVEY methods in SAS version 9.3 (SAS Institute) and checked for multicollinearity with the Belsley-Kuh-Welsch technique. Finally, we used the American Hospital Association (AHA) database for analyzing substance use rehabilitation availability on per hospital basis.
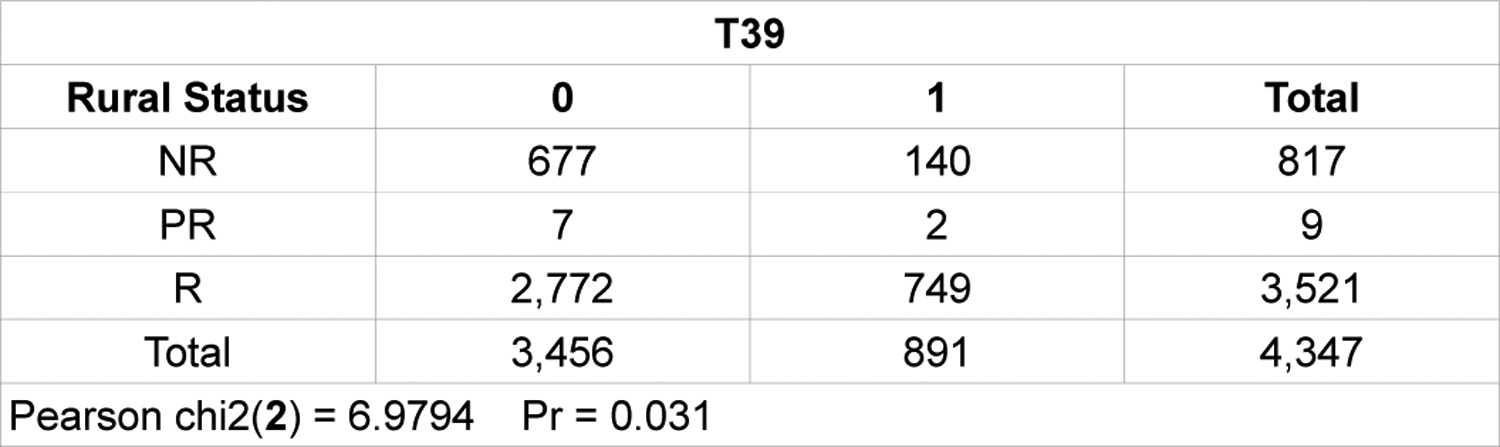
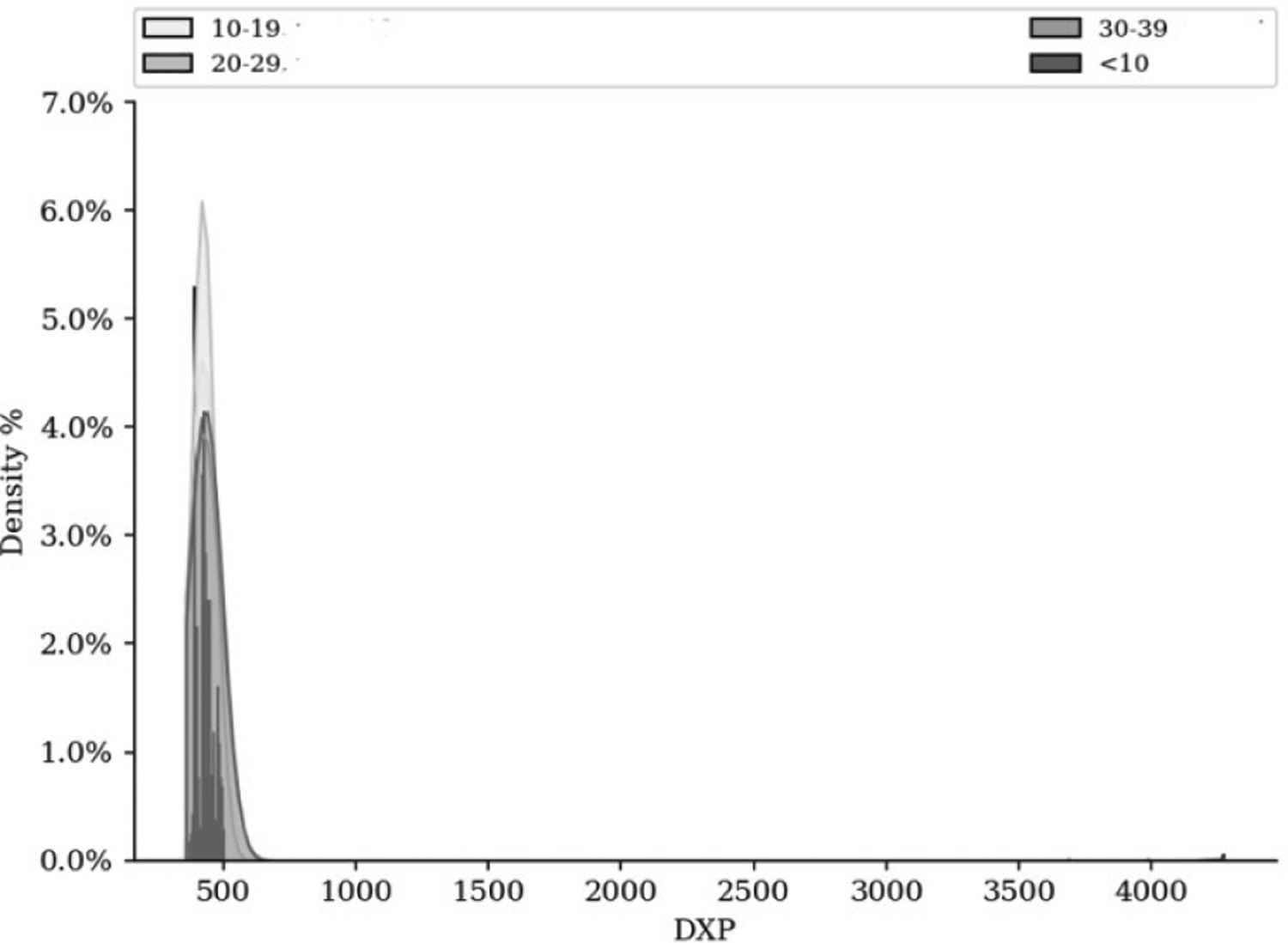
Results: The chi-square statistic for comparing opioid codes against non-opioid codes distributed among three categories, rural, non-rural, and partially rural was significant at the limit of p <0.05. 81.134% of opioid-led poisoning codes were activated in a rural county. Only four hospitals had substance-use rehabilitation, three of which were in a non-rural area. More people from the teenage and early-adulthood years (10-19) were prone to opioid usage.
Conclusions: Rural counties in South Dakota were more likely to dispense opioid care and not have access to rehabilitation. We also found that as the opioid dispensing rate at hospitals within a state decreased as the state had less rural counties. Introducing public programs to train more physicians and cutting down cost of non-opioid based care may lower opioid distribution and increase rehabilitation options in rural hospitals.
 分享
分享



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
