{"title":"NMR-based serum and muscle metabolomics for diagnosis and activity assessment in idiopathic inflammatory myopathies","authors":"Anupam Guleria, Umesh Kumar, Dinesh Kumar, Naveen R, Anamika Kumari Anuja, Mantabya Kumar Singh, Pulak Sharma, Vikas Agarwal, Ramnath Misra, Latika Gupta","doi":"10.1002/ansa.202000171","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objectives</h3>\n \n <p>Differentiating smoldering disease activity from weakness due to fatty replacement of atrophied muscle can often be a challenge in the idiopathic inflammatory myositis (IIM). We aimed to identify the metabolic disturbances associated with IIM and if these changes can aid in the assessment of disease activity.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Metabolic profiles of sera (N = 99) and muscle (N = 21) from patients with IIM (ACR-EULAR criteria) were compared with healthy control (HC) samples (N = 75 for serum and N = 12 for muscle tissues) employing 800 MHz NMR (Nuclear Magnetic Resonance) spectroscopy. Metabolic disparity between IIM and HC was established based on Partial Least Squares Discriminant Analysis (PLS-DA) and the discriminatory metabolites were identified based on variable importance in projection (VIP) statistics (<i>P</i>-value < .05, corrected for false discovery rate (FDR)).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Serum metabolomics profiles were distinctive in IIM as compared to HC, with a visible shift to anaerobic metabolism (increased lactate, low glucose), oxidative defect (high Phenylalanine/tyrosine), decreased muscle mass (low serum creatinine), increased muscle catabolism (increased branched-chain amino acids), and dyslipidemia (higher lipids, higher very low-density lipoprotein [VLDL]/low-density lipoprotein [LDL] ratio, lower polyunsaturated fatty acid [PUFA]). The sera of active IIM patients were characterized by anaerobic metabolism (low glucose), loss of muscle mass (low creatinine, amino acids), and oxidative defect (high Phenylalanine/tyrosine). Three metabolites (isopropanol, succinate, and glycine) were distinctive in muscle tissue metabolomics. NMR-based serum metabolic disparity was lacking between different clinical subsets of IIM.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Serum and muscle tissue metabolomics have the potential to distinguish (a) IIM from HC and (b) active IIM from inactive IIM irrespective of disease subtype.</p>\n </section>\n </div>","PeriodicalId":93411,"journal":{"name":"Analytical science advances","volume":"2 11-12","pages":"515-526"},"PeriodicalIF":4.1000,"publicationDate":"2021-06-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/ansa.202000171","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Analytical science advances","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ansa.202000171","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CHEMISTRY, ANALYTICAL","Score":null,"Total":0}
引用次数: 6
Abstract
Objectives
Differentiating smoldering disease activity from weakness due to fatty replacement of atrophied muscle can often be a challenge in the idiopathic inflammatory myositis (IIM). We aimed to identify the metabolic disturbances associated with IIM and if these changes can aid in the assessment of disease activity.
Methods
Metabolic profiles of sera (N = 99) and muscle (N = 21) from patients with IIM (ACR-EULAR criteria) were compared with healthy control (HC) samples (N = 75 for serum and N = 12 for muscle tissues) employing 800 MHz NMR (Nuclear Magnetic Resonance) spectroscopy. Metabolic disparity between IIM and HC was established based on Partial Least Squares Discriminant Analysis (PLS-DA) and the discriminatory metabolites were identified based on variable importance in projection (VIP) statistics (P-value < .05, corrected for false discovery rate (FDR)).
Results
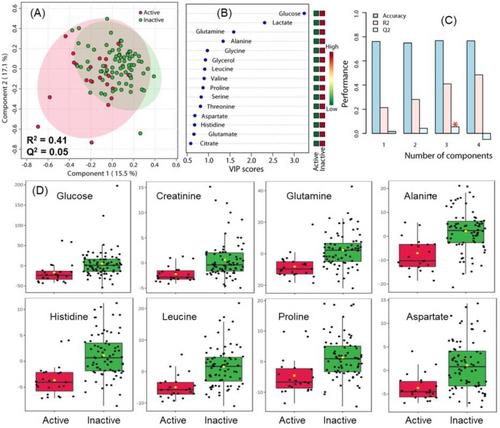
Serum metabolomics profiles were distinctive in IIM as compared to HC, with a visible shift to anaerobic metabolism (increased lactate, low glucose), oxidative defect (high Phenylalanine/tyrosine), decreased muscle mass (low serum creatinine), increased muscle catabolism (increased branched-chain amino acids), and dyslipidemia (higher lipids, higher very low-density lipoprotein [VLDL]/low-density lipoprotein [LDL] ratio, lower polyunsaturated fatty acid [PUFA]). The sera of active IIM patients were characterized by anaerobic metabolism (low glucose), loss of muscle mass (low creatinine, amino acids), and oxidative defect (high Phenylalanine/tyrosine). Three metabolites (isopropanol, succinate, and glycine) were distinctive in muscle tissue metabolomics. NMR-based serum metabolic disparity was lacking between different clinical subsets of IIM.
Conclusion
Serum and muscle tissue metabolomics have the potential to distinguish (a) IIM from HC and (b) active IIM from inactive IIM irrespective of disease subtype.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
