Non-invasive left ventricular pressure-volume loops from cardiovascular magnetic resonance imaging and brachial blood pressure: validation using pressure catheter measurements.
Per M Arvidsson, Peregrine G Green, William D Watson, Mayooran Shanmuganathan, Einar Heiberg, Giovanni Luigi De Maria, Håkan Arheden, Neil Herring, Oliver J Rider
{"title":"Non-invasive left ventricular pressure-volume loops from cardiovascular magnetic resonance imaging and brachial blood pressure: validation using pressure catheter measurements.","authors":"Per M Arvidsson, Peregrine G Green, William D Watson, Mayooran Shanmuganathan, Einar Heiberg, Giovanni Luigi De Maria, Håkan Arheden, Neil Herring, Oliver J Rider","doi":"10.1093/ehjimp/qyad035","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Left ventricular (LV) pressure-volume (PV) loops provide gold-standard physiological information but require invasive measurements of ventricular intracavity pressure, limiting clinical and research applications. A non-invasive method for the computation of PV loops from magnetic resonance imaging and brachial cuff blood pressure has recently been proposed. Here we evaluated the fidelity of the non-invasive PV algorithm against invasive LV pressures in humans.</p><p><strong>Methods and results: </strong>Four heart failure patients with EF < 35% and LV dyssynchrony underwent cardiovascular magnetic resonance (CMR) imaging and subsequent LV catheterization with sequential administration of two different intravenous metabolic substrate infusions (insulin/dextrose and lipid emulsion), producing eight datasets at different haemodynamic states. Pressure-volume loops were computed from CMR volumes combined with (i) a time-varying elastance function scaled to brachial blood pressure and temporally stretched to match volume data, or (ii) invasive pressures averaged from 19 to 30 sampled beats. Method comparison was conducted using linear regression and Bland-Altman analysis. Non-invasively derived PV loop parameters demonstrated high correlation and low bias when compared to invasive data for stroke work (R<sup>2</sup> = 0.96, <i>P</i> < 0.0001, bias 4.6%), potential energy (R<sup>2</sup> = 0.83, <i>P</i> = 0.001, bias 1.5%), end-systolic pressure-volume relationship (R<sup>2</sup> = 0.89, <i>P</i> = 0.0004, bias 5.8%), ventricular efficiency (R<sup>2</sup> = 0.98, <i>P</i> < 0.0001, bias 0.8%), arterial elastance (R<sup>2</sup> = 0.88, <i>P</i> = 0.0006, bias -8.0%), mean external power (R<sup>2</sup> = 0.92, <i>P</i> = 0.0002, bias 4.4%), and energy per ejected volume (R<sup>2</sup> = 0.89, <i>P</i> = 0.0001, bias 3.7%). Variations in estimated end-diastolic pressure did not significantly affect results (<i>P</i> > 0.05 for all). Intraobserver analysis after one year demonstrated 0.9-3.4% bias for LV volumetry and 0.2-5.4% for PV loop-derived parameters.</p><p><strong>Conclusion: </strong>Pressure-volume loops can be precisely and accurately computed from CMR imaging and brachial cuff blood pressure in humans.</p>","PeriodicalId":94317,"journal":{"name":"European heart journal. Imaging methods and practice","volume":"1 2","pages":"qyad035"},"PeriodicalIF":0.0000,"publicationDate":"2023-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10631830/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Imaging methods and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjimp/qyad035","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Left ventricular (LV) pressure-volume (PV) loops provide gold-standard physiological information but require invasive measurements of ventricular intracavity pressure, limiting clinical and research applications. A non-invasive method for the computation of PV loops from magnetic resonance imaging and brachial cuff blood pressure has recently been proposed. Here we evaluated the fidelity of the non-invasive PV algorithm against invasive LV pressures in humans.
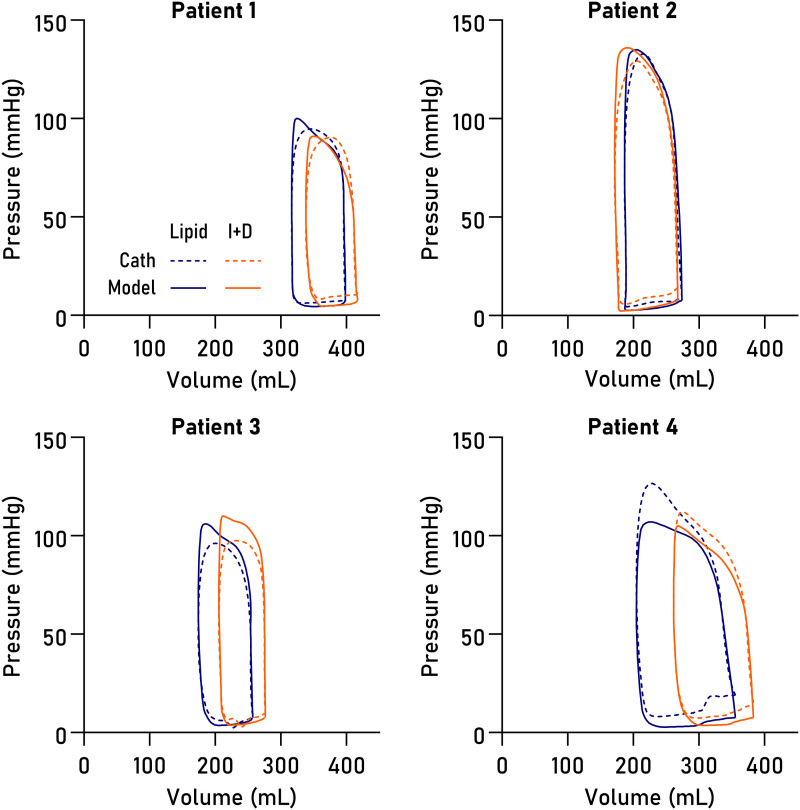
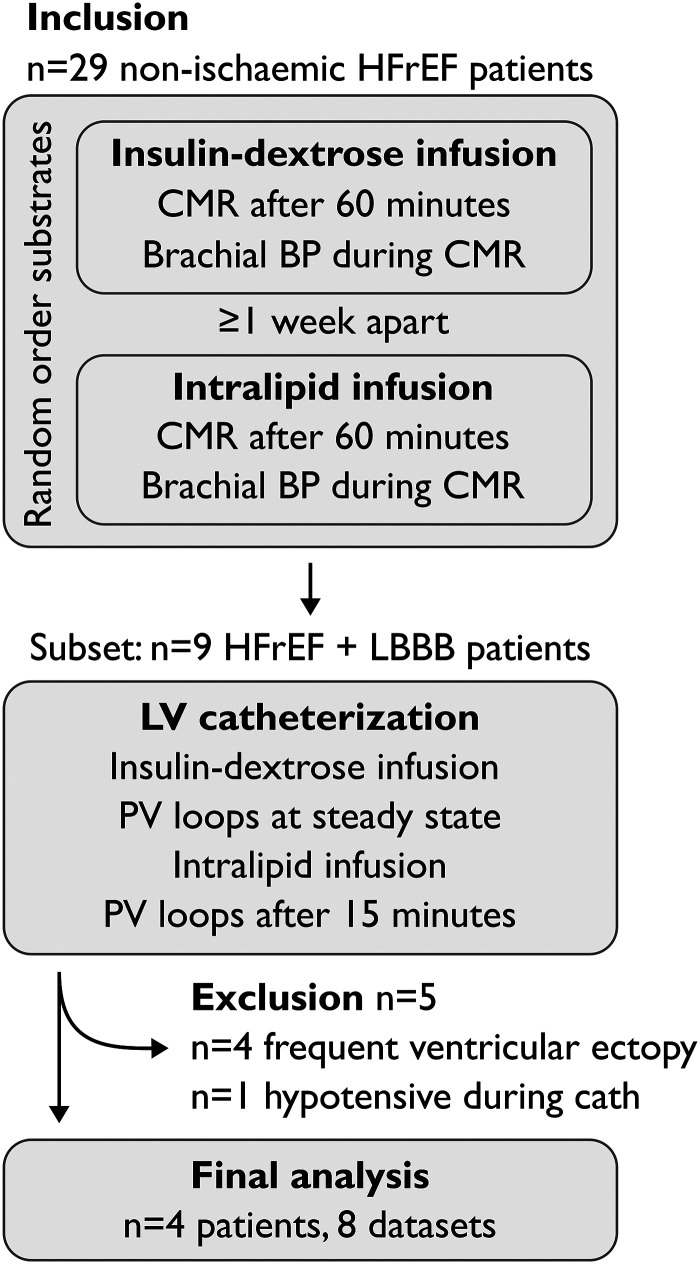
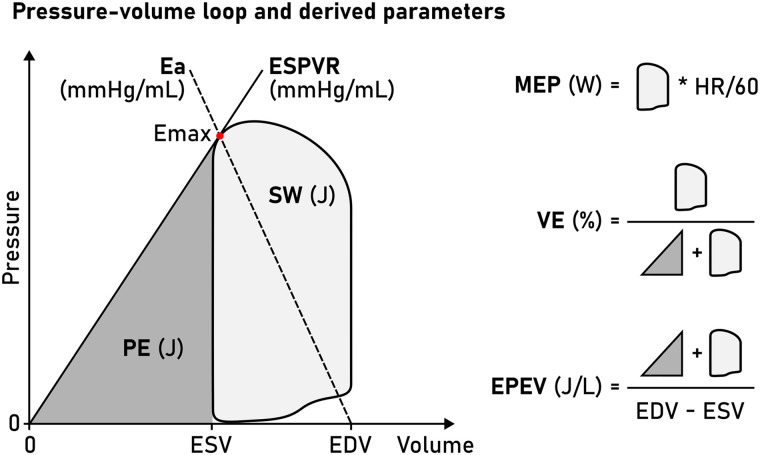
Methods and results: Four heart failure patients with EF < 35% and LV dyssynchrony underwent cardiovascular magnetic resonance (CMR) imaging and subsequent LV catheterization with sequential administration of two different intravenous metabolic substrate infusions (insulin/dextrose and lipid emulsion), producing eight datasets at different haemodynamic states. Pressure-volume loops were computed from CMR volumes combined with (i) a time-varying elastance function scaled to brachial blood pressure and temporally stretched to match volume data, or (ii) invasive pressures averaged from 19 to 30 sampled beats. Method comparison was conducted using linear regression and Bland-Altman analysis. Non-invasively derived PV loop parameters demonstrated high correlation and low bias when compared to invasive data for stroke work (R2 = 0.96, P < 0.0001, bias 4.6%), potential energy (R2 = 0.83, P = 0.001, bias 1.5%), end-systolic pressure-volume relationship (R2 = 0.89, P = 0.0004, bias 5.8%), ventricular efficiency (R2 = 0.98, P < 0.0001, bias 0.8%), arterial elastance (R2 = 0.88, P = 0.0006, bias -8.0%), mean external power (R2 = 0.92, P = 0.0002, bias 4.4%), and energy per ejected volume (R2 = 0.89, P = 0.0001, bias 3.7%). Variations in estimated end-diastolic pressure did not significantly affect results (P > 0.05 for all). Intraobserver analysis after one year demonstrated 0.9-3.4% bias for LV volumetry and 0.2-5.4% for PV loop-derived parameters.
Conclusion: Pressure-volume loops can be precisely and accurately computed from CMR imaging and brachial cuff blood pressure in humans.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
