Cynthia M Boyd, Susan M Shetterly, John D Powers, Linda A Weffald, Ariel R Green, Orla C Sheehan, Emily Reeve, Melanie L Drace, Jonathan D Norton, Mahesh Maiyani, Kathy S Gleason, Jennifer K Sawyer, Matthew L Maciejewski, Jennifer L Wolff, Courtney Kraus, Elizabeth A Bayliss
{"title":"Evaluating the Safety of an Educational Deprescribing Intervention: Lessons from the Optimize Trial.","authors":"Cynthia M Boyd, Susan M Shetterly, John D Powers, Linda A Weffald, Ariel R Green, Orla C Sheehan, Emily Reeve, Melanie L Drace, Jonathan D Norton, Mahesh Maiyani, Kathy S Gleason, Jennifer K Sawyer, Matthew L Maciejewski, Jennifer L Wolff, Courtney Kraus, Elizabeth A Bayliss","doi":"10.1007/s40266-023-01080-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients, family members, and clinicians express concerns about potential adverse drug withdrawal events (ADWEs) following medication discontinuation or fears of upsetting a stable medical equilibrium as key barriers to deprescribing. Currently, there are limited methods to pragmatically assess the safety of deprescribing and ascertain ADWEs. We report the methods and results of safety monitoring for the OPTIMIZE trial of deprescribing education for patients, family members, and clinicians.</p><p><strong>Methods: </strong>This was a pragmatic cluster randomized trial with multivariable Poisson regression comparing outcome rates between study arms. We conducted clinical record review and adjudication of sampled records to assess potential causal relationships between medication discontinuation and outcomes. This study included adults aged 65+ with dementia or mild cognitive impairment, one or more additional chronic conditions, and prescribed 5+ chronic medications. The intervention included an educational brochure on deprescribing that was mailed to patients prior to primary care visits, a clinician notification about individual brochure mailings, and an educational tip sheets was provided monthly to primary care clinicians. The outcomes of the safety monitoring were rates of hospitalizations and mortality during the 4 months following brochure mailings and results of record review and adjudication. The adjudication process was conducted throughout the trial and included classifications: likely, possibly, and unlikely.</p><p><strong>Results: </strong>There was a total of 3012 (1433 intervention and 1579 control) participants. There were 420 total hospitalizations involving 269 (18.8%) people in the intervention versus 517 total hospitalizations involving 317 (20.1%) people in the control groups. Adjusted risk ratios comparing intervention to control groups were 0.92 [95% confidence interval (CI) 0.72, 1.16] for hospitalization and 1.19 (95% CI 0.67, 2.11) for mortality. Both groups had zero deaths \"likely\" attributed to a medication change prior to the event. A total of 3 out of 30 (10%) intervention group hospitalizations and 7 out of 35 (20%) control group hospitalizations were considered \"likely\" due to a medication change.</p><p><strong>Conclusions: </strong>Population-based deprescribing education is safe in the older adult population with cognitive impairment in our study. Pragmatic methods for safety monitoring are needed to further inform deprescribing interventions.</p><p><strong>Trial registration: </strong>NCT03984396. Registered on 13 June 2019.</p>","PeriodicalId":11489,"journal":{"name":"Drugs & Aging","volume":" ","pages":"45-54"},"PeriodicalIF":3.8000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11101016/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drugs & Aging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40266-023-01080-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/20 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients, family members, and clinicians express concerns about potential adverse drug withdrawal events (ADWEs) following medication discontinuation or fears of upsetting a stable medical equilibrium as key barriers to deprescribing. Currently, there are limited methods to pragmatically assess the safety of deprescribing and ascertain ADWEs. We report the methods and results of safety monitoring for the OPTIMIZE trial of deprescribing education for patients, family members, and clinicians.
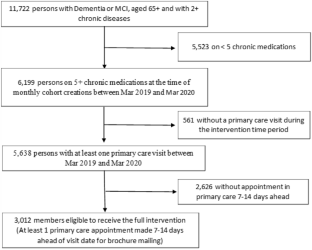
Methods: This was a pragmatic cluster randomized trial with multivariable Poisson regression comparing outcome rates between study arms. We conducted clinical record review and adjudication of sampled records to assess potential causal relationships between medication discontinuation and outcomes. This study included adults aged 65+ with dementia or mild cognitive impairment, one or more additional chronic conditions, and prescribed 5+ chronic medications. The intervention included an educational brochure on deprescribing that was mailed to patients prior to primary care visits, a clinician notification about individual brochure mailings, and an educational tip sheets was provided monthly to primary care clinicians. The outcomes of the safety monitoring were rates of hospitalizations and mortality during the 4 months following brochure mailings and results of record review and adjudication. The adjudication process was conducted throughout the trial and included classifications: likely, possibly, and unlikely.
Results: There was a total of 3012 (1433 intervention and 1579 control) participants. There were 420 total hospitalizations involving 269 (18.8%) people in the intervention versus 517 total hospitalizations involving 317 (20.1%) people in the control groups. Adjusted risk ratios comparing intervention to control groups were 0.92 [95% confidence interval (CI) 0.72, 1.16] for hospitalization and 1.19 (95% CI 0.67, 2.11) for mortality. Both groups had zero deaths "likely" attributed to a medication change prior to the event. A total of 3 out of 30 (10%) intervention group hospitalizations and 7 out of 35 (20%) control group hospitalizations were considered "likely" due to a medication change.
Conclusions: Population-based deprescribing education is safe in the older adult population with cognitive impairment in our study. Pragmatic methods for safety monitoring are needed to further inform deprescribing interventions.
Trial registration: NCT03984396. Registered on 13 June 2019.
期刊介绍:
Drugs & Aging delivers essential information on the most important aspects of drug therapy to professionals involved in the care of the elderly.
The journal addresses in a timely way the major issues relating to drug therapy in older adults including: the management of specific diseases, particularly those associated with aging, age-related physiological changes impacting drug therapy, drug utilization and prescribing in the elderly, polypharmacy and drug interactions.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
