{"title":"Is the anterior approach recommended for liver resection of hepatocellular carcinoma? A systematic review and meta-analysis","authors":"Takamichi Ishii, Kentaro Iwaki, Akiyoshi Nakakura, Yoichiro Uchida, Takashi Ito, Etsuro Hatano","doi":"10.1002/jhbp.1393","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background/Purpose</h3>\n \n <p>The anterior approach (AA) in liver resection has proven more effective with regard to short-term outcomes than the conventional approach (CA). However, its superiority over the CA concerning long-term outcomes remains unclear. This meta-analysis compared the short- and long-term outcomes of the AA and CA.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Databases, including MEDLINE, Web of Science, and Cochrane Central Register of Controlled Trials, were searched to identify studies comparing the AA and CA for hepatocellular carcinoma (HCC) liver resection. The primary outcomes were the in-hospital mortality, in-hospital morbidity, disease-free survival (DFS), and overall survival (OS). Secondary outcomes were operative time, blood loss, blood transfusion, R0 rate, and length of hospital stay.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Ten studies involving 1369 patients were included (AA, <i>n</i> = 595; CA, <i>n</i> = 774). Despite no significant differences in the in-hospital mortality or morbidity, the AA demonstrated a superior DFS (hazard ratio [HR], 0.63; 95% confidence interval [CI]: 0.51–0.77) and OS (HR, 0.56; 95% CI: 0.48–0.65) and was associated with a longer operative time, less blood loss, and less transfusion than the CA. No marked differences in other outcomes were noted.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>The AA for HCC liver resection helped reduce blood loss and need for transfusion, improving the DFS and OS.</p>\n </section>\n </div>","PeriodicalId":16056,"journal":{"name":"Journal of Hepato‐Biliary‐Pancreatic Sciences","volume":"31 3","pages":"133-142"},"PeriodicalIF":2.8000,"publicationDate":"2023-11-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jhbp.1393","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepato‐Biliary‐Pancreatic Sciences","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jhbp.1393","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background/Purpose
The anterior approach (AA) in liver resection has proven more effective with regard to short-term outcomes than the conventional approach (CA). However, its superiority over the CA concerning long-term outcomes remains unclear. This meta-analysis compared the short- and long-term outcomes of the AA and CA.
Methods
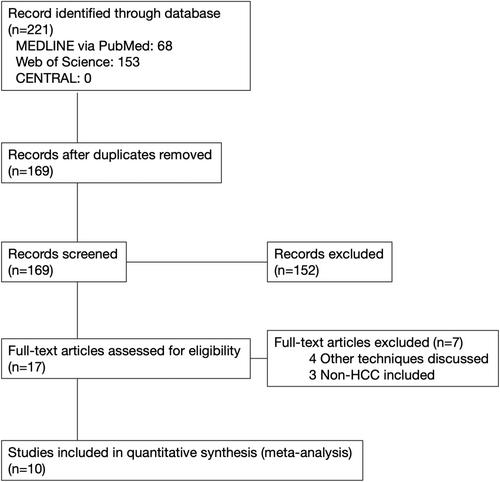
Databases, including MEDLINE, Web of Science, and Cochrane Central Register of Controlled Trials, were searched to identify studies comparing the AA and CA for hepatocellular carcinoma (HCC) liver resection. The primary outcomes were the in-hospital mortality, in-hospital morbidity, disease-free survival (DFS), and overall survival (OS). Secondary outcomes were operative time, blood loss, blood transfusion, R0 rate, and length of hospital stay.
Results
Ten studies involving 1369 patients were included (AA, n = 595; CA, n = 774). Despite no significant differences in the in-hospital mortality or morbidity, the AA demonstrated a superior DFS (hazard ratio [HR], 0.63; 95% confidence interval [CI]: 0.51–0.77) and OS (HR, 0.56; 95% CI: 0.48–0.65) and was associated with a longer operative time, less blood loss, and less transfusion than the CA. No marked differences in other outcomes were noted.
Conclusions
The AA for HCC liver resection helped reduce blood loss and need for transfusion, improving the DFS and OS.
背景/目的:肝切除术的前路(AA)已被证明在短期预后方面比传统入路(CA)更有效。然而,就长期结果而言,其优于CA的优势尚不清楚。本荟萃分析比较了AA和CA的短期和长期结果。方法:检索数据库,包括MEDLINE、Web of Science和Cochrane中央对照试验注册库,以确定比较AA和CA在肝细胞癌(HCC)肝切除术中的研究。主要结局是院内死亡率、院内发病率、无病生存期(DFS)和总生存期(OS)。次要结局为手术时间、出血量、输血量、R0率和住院时间。结果:纳入10项研究,共1369例患者(AA, n = 595;CA, n = 774)。尽管两组在住院死亡率和发病率方面没有显著差异,但AA组表现出更高的DFS(风险比[HR], 0.63;95%可信区间[CI]: 0.51-0.77)和OS (HR, 0.56;95% CI: 0.48-0.65),与CA相比,手术时间更长,出血量更少,输血量更少。其他结果无显著差异。结论:肝细胞癌肝切除术AA可减少出血量和输血需求,改善DFS和OS。
期刊介绍:
The Journal of Hepato-Biliary-Pancreatic Sciences (JHBPS) is the leading peer-reviewed journal in the field of hepato-biliary-pancreatic sciences. JHBPS publishes articles dealing with clinical research as well as translational research on all aspects of this field. Coverage includes Original Article, Review Article, Images of Interest, Rapid Communication and an announcement section. Letters to the Editor and comments on the journal’s policies or content are also included. JHBPS welcomes submissions from surgeons, physicians, endoscopists, radiologists, oncologists, and pathologists.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
