Thrombolysis with Recombinant Human Prourokinase 4.5-6 h After Acute Ischemic Stroke: A Phase IIa, Randomized, and Open-Label Multicenter Clinical Trial.
Haiqing Song, Yuan Wang, Qingfeng Ma, Huisheng Chen, Bo Liu, Yi Yang, Jianguo Zhu, Shigang Zhao, Xiaoping Jin, Yongqiu Li, Yanyong Wang, Runxiu Zhu, Liandong Zhao, Junyan Liu, Wuwei Feng, Rui Liu, Xunming Ji, Yuping Wang
{"title":"Thrombolysis with Recombinant Human Prourokinase 4.5-6 h After Acute Ischemic Stroke: A Phase IIa, Randomized, and Open-Label Multicenter Clinical Trial.","authors":"Haiqing Song, Yuan Wang, Qingfeng Ma, Huisheng Chen, Bo Liu, Yi Yang, Jianguo Zhu, Shigang Zhao, Xiaoping Jin, Yongqiu Li, Yanyong Wang, Runxiu Zhu, Liandong Zhao, Junyan Liu, Wuwei Feng, Rui Liu, Xunming Ji, Yuping Wang","doi":"10.1007/s40263-023-01051-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ischemic stroke is a major cause of disability and death worldwide. A narrow therapeutic window profoundly constrained the utilization of alteplase.</p><p><strong>Objectives: </strong>To investigate therapeutic effects and safety of intravenous recombinant human prourokinase (rhPro-UK) in patients with acute ischemic stroke (AIS) in the 4.5-6 h therapeutic time windows.</p><p><strong>Methods: </strong>We conducted a phase IIa, randomized, and open-label multicenter clinical trial. Between 4.5 and 6 h after the onset of AIS, patients were randomly administrated to receive intravenous rhPro-UK at a 50 mg or 35 mg dose. The primary endpoint was excellent functional outcome defined as modified Rankin scale (mRS) score of 1 or less at 90 days. The secondary outcome was the treatment response, which was based on an at least 4-point improvement from baseline National Institutes of Health stroke scale (NIHSS) score at 24 h after drug administration. Safety endpoints included death, symptomatic intracerebral hemorrhage (sICH), and other serious adverse events.</p><p><strong>Results: </strong>We enrolled 80 patients in the 4.5-6 h therapeutic time windows at 17 medical centers in China from December 2016 to November 2017. A total of 39 patients were treated with 50 mg rhPro-UK, and 39 were treated with 35 mg rhPro-UK. Compared with the baseline, the NIHSS score at 24 h and days 7, 14, 30, and 90 was decreased significantly among patients treated with either rhPro-UK 50 mg or 35 mg. The mean reduction in the NIHSS from baseline to 90 days after the onset was 3.56 and 5.79 in the rhPro-UK 50 mg group and the rhPro-UK 35 mg group, respectively. The rates of functional independence at 90 days of rhPro-UK 50 mg and 35 mg were 61.54% and 69.23%, respectively (P = 0.475), and the proportion of patients with functional response to treatment at 24 h were 28.21% and 33.33% (P = 0.624). No sICH occurred in the two groups, and death occurred in only one patient in the rhPro-UK 50 mg group. There was no significant difference in mortality at 90 days and the rate of other serious adverse events between two groups.</p><p><strong>Conclusion: </strong>In the 4.5-6 h time window, more than 60% of patients at either dose of rhPro-UK (50 mg or 35 mg) achieved functional independence at 90 days without increased mortality and sICH risk. Thus, intravenous rhPro-UK was effective and safe for patients with AIS within 4.5-6 h after stroke onset. While no significant differences were identified between different dosages of rhPro-UK regarding clinical outcomes, it is a logical step to further test the safety and efficacy of the low dose of rhPro-UK in a well-powered phase III study.</p><p><strong>Trial registration: </strong>http://www.chictr.org.cn . Identifier: ChiCTR1800016519. Date of registration: 6 June 2018.</p>","PeriodicalId":10508,"journal":{"name":"CNS drugs","volume":" ","pages":"67-75"},"PeriodicalIF":7.4000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10811005/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CNS drugs","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40263-023-01051-2","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/29 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Ischemic stroke is a major cause of disability and death worldwide. A narrow therapeutic window profoundly constrained the utilization of alteplase.
Objectives: To investigate therapeutic effects and safety of intravenous recombinant human prourokinase (rhPro-UK) in patients with acute ischemic stroke (AIS) in the 4.5-6 h therapeutic time windows.
Methods: We conducted a phase IIa, randomized, and open-label multicenter clinical trial. Between 4.5 and 6 h after the onset of AIS, patients were randomly administrated to receive intravenous rhPro-UK at a 50 mg or 35 mg dose. The primary endpoint was excellent functional outcome defined as modified Rankin scale (mRS) score of 1 or less at 90 days. The secondary outcome was the treatment response, which was based on an at least 4-point improvement from baseline National Institutes of Health stroke scale (NIHSS) score at 24 h after drug administration. Safety endpoints included death, symptomatic intracerebral hemorrhage (sICH), and other serious adverse events.
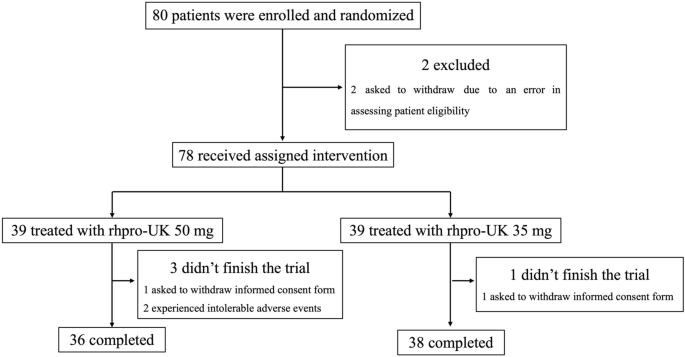
Results: We enrolled 80 patients in the 4.5-6 h therapeutic time windows at 17 medical centers in China from December 2016 to November 2017. A total of 39 patients were treated with 50 mg rhPro-UK, and 39 were treated with 35 mg rhPro-UK. Compared with the baseline, the NIHSS score at 24 h and days 7, 14, 30, and 90 was decreased significantly among patients treated with either rhPro-UK 50 mg or 35 mg. The mean reduction in the NIHSS from baseline to 90 days after the onset was 3.56 and 5.79 in the rhPro-UK 50 mg group and the rhPro-UK 35 mg group, respectively. The rates of functional independence at 90 days of rhPro-UK 50 mg and 35 mg were 61.54% and 69.23%, respectively (P = 0.475), and the proportion of patients with functional response to treatment at 24 h were 28.21% and 33.33% (P = 0.624). No sICH occurred in the two groups, and death occurred in only one patient in the rhPro-UK 50 mg group. There was no significant difference in mortality at 90 days and the rate of other serious adverse events between two groups.
Conclusion: In the 4.5-6 h time window, more than 60% of patients at either dose of rhPro-UK (50 mg or 35 mg) achieved functional independence at 90 days without increased mortality and sICH risk. Thus, intravenous rhPro-UK was effective and safe for patients with AIS within 4.5-6 h after stroke onset. While no significant differences were identified between different dosages of rhPro-UK regarding clinical outcomes, it is a logical step to further test the safety and efficacy of the low dose of rhPro-UK in a well-powered phase III study.
Trial registration: http://www.chictr.org.cn . Identifier: ChiCTR1800016519. Date of registration: 6 June 2018.
期刊介绍:
CNS Drugs promotes rational pharmacotherapy within the disciplines of clinical psychiatry and neurology. The Journal includes:
- Overviews of contentious or emerging issues.
- Comprehensive narrative reviews that provide an authoritative source of information on pharmacological approaches to managing neurological and psychiatric illnesses.
- Systematic reviews that collate empirical evidence to answer a specific research question, using explicit, systematic methods as outlined by the PRISMA statement.
- Adis Drug Reviews of the properties and place in therapy of both newer and established drugs in neurology and psychiatry.
- Original research articles reporting the results of well-designed studies with a strong link to clinical practice, such as clinical pharmacodynamic and pharmacokinetic studies, clinical trials, meta-analyses, outcomes research, and pharmacoeconomic and pharmacoepidemiological studies.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in CNS Drugs may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
