The Impact of Missing Postoperative Longitudinal Pain Data on Study Results Investigating Analgesia from Transversus Abdominis Plane Block on Postoperative Day One Following Abdominal Surgery: A Single-Center Retrospective Chart Review.
{"title":"The Impact of Missing Postoperative Longitudinal Pain Data on Study Results Investigating Analgesia from Transversus Abdominis Plane Block on Postoperative Day One Following Abdominal Surgery: A Single-Center Retrospective Chart Review.","authors":"James Harvey Jones","doi":"10.2147/LRA.S439429","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aims of this study are to analyze the association between the number of recorded pain scores and baseline pain following surgery, analgesia technique, and patient demographics, as well as the substitution of missing data with the results from mean substitution, last observation carried forward, regression imputation, multiple imputation, and mixed models.</p><p><strong>Methods: </strong>This retrospective chart review was approved by the Institutional Review Board (IRB). The following data were collected: patient demographics (age, gender, body mass index (BMI), race, and ethnicity); surgery type and date; analgesia with or without transversus abdominis plane (TAP) block; as well as the time, date, and value for all postoperative pain scores on the first postoperative day (POD). The following null hypotheses were tested: (1) the number of pain recordings will be independent of TAP block analgesia, baseline pain on POD 1, and patient demographics; and (2) there will be no significant differences in pain scores with and without TAP block analgesia following complete case analysis, mean substitution, last observation carried forward, regression imputation, multiple imputation, and mixed models.</p><p><strong>Results: </strong>This study analyzed 486 patients including 2562 recorded pain scores. An increase in age by one year is, on average, associated with a 0.04 (95% confidence interval (CI) -0.060 to -0.025) decrease in the number of pain scores recorded (p < 0.001). Black race is associated with 0.763 less pain scores, on average (95% CI -1.49 to -0.039) and this value is statistically significant (p = 0.039). All datasets with substituted values for missing data yield lower pain scores for patients who did not receive TAP block. Significant differences in recorded pain scores are only noted for scores recorded between 0400 and 0759 and 1600-1959 in mixed models.</p><p><strong>Conclusion: </strong>Discrepancies in pain score recordings among patients are associated with age and black race. When these discrepancies are addressed with statistical methods, clinically significant differences are appreciated.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"16 ","pages":"173-182"},"PeriodicalIF":1.9000,"publicationDate":"2023-11-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10695121/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S439429","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The aims of this study are to analyze the association between the number of recorded pain scores and baseline pain following surgery, analgesia technique, and patient demographics, as well as the substitution of missing data with the results from mean substitution, last observation carried forward, regression imputation, multiple imputation, and mixed models.
Methods: This retrospective chart review was approved by the Institutional Review Board (IRB). The following data were collected: patient demographics (age, gender, body mass index (BMI), race, and ethnicity); surgery type and date; analgesia with or without transversus abdominis plane (TAP) block; as well as the time, date, and value for all postoperative pain scores on the first postoperative day (POD). The following null hypotheses were tested: (1) the number of pain recordings will be independent of TAP block analgesia, baseline pain on POD 1, and patient demographics; and (2) there will be no significant differences in pain scores with and without TAP block analgesia following complete case analysis, mean substitution, last observation carried forward, regression imputation, multiple imputation, and mixed models.
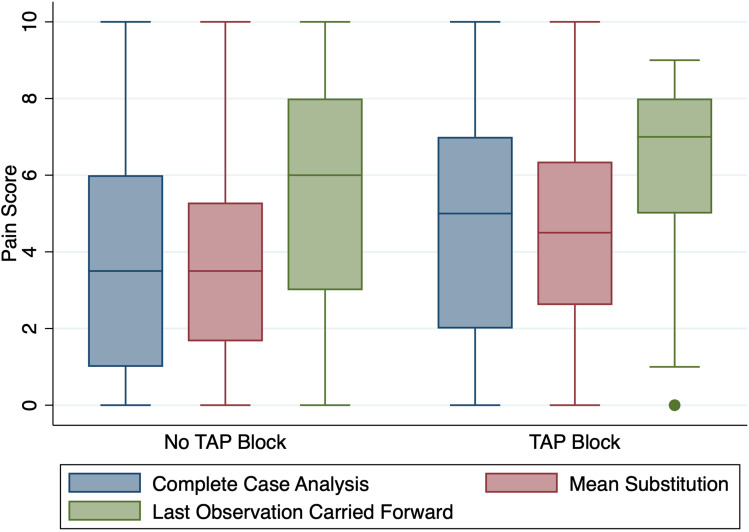
Results: This study analyzed 486 patients including 2562 recorded pain scores. An increase in age by one year is, on average, associated with a 0.04 (95% confidence interval (CI) -0.060 to -0.025) decrease in the number of pain scores recorded (p < 0.001). Black race is associated with 0.763 less pain scores, on average (95% CI -1.49 to -0.039) and this value is statistically significant (p = 0.039). All datasets with substituted values for missing data yield lower pain scores for patients who did not receive TAP block. Significant differences in recorded pain scores are only noted for scores recorded between 0400 and 0759 and 1600-1959 in mixed models.
Conclusion: Discrepancies in pain score recordings among patients are associated with age and black race. When these discrepancies are addressed with statistical methods, clinically significant differences are appreciated.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
