Allison L Skinner-Dorkenoo, Kasheena G Rogbeer, Apoorva Sarmal, Cynthia Ware, Jennifer Zhu
{"title":"Challenging Race-Based Medicine Through Historical Education About the Social Construction of Race.","authors":"Allison L Skinner-Dorkenoo, Kasheena G Rogbeer, Apoorva Sarmal, Cynthia Ware, Jennifer Zhu","doi":"10.1089/heq.2023.0036","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Scientifically, there is little genetic variation among humans and race has no biological basis. However, medical school preclinical curricula tend to misrepresent race and reify biologically essentialist explanations for disease. The social construct of race is, therefore, used to inform health care providers' treatment decisions. Use of race-based medicine has been identified as a contributor to racial health disparities, spurring a growing movement to challenge race essentialism and race-based medicine. The current research tested an intervention that educates college students about the historical construction of racial categories in the United States.</p><p><strong>Methods: </strong>Participants who were randomly assigned to the intervention condition read an article highlighting the history of the sociopolitical construction of race. They were then prompted to discuss in dyads how racial categories were created and changed over history, and-in light of all this-the appropriateness of race-based medicine. Those assigned to the control condition advanced directly to the outcome measures.</p><p><strong>Results: </strong>Participants in the intervention condition reported less race essentialism, less support for race-based medicine, and greater belief that race-based medicine contributes to racial health disparities. Findings were not moderated by premed status.</p><p><strong>Discussion: </strong>Our data provide initial evidence that our interactive intervention could effectively reduce biological essentialism and support for race-based medicine in both premed and non-premed students.</p><p><strong>Health equity implications: </strong>This intervention has the potential to shape the way health care providers in-training understand race, their internalization of biologically essentialist explanations for disease, and willingness to adopt race-based treatment plans.</p>","PeriodicalId":36602,"journal":{"name":"Health Equity","volume":"7 1","pages":"764-772"},"PeriodicalIF":2.5000,"publicationDate":"2023-11-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10698761/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Equity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/heq.2023.0036","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Scientifically, there is little genetic variation among humans and race has no biological basis. However, medical school preclinical curricula tend to misrepresent race and reify biologically essentialist explanations for disease. The social construct of race is, therefore, used to inform health care providers' treatment decisions. Use of race-based medicine has been identified as a contributor to racial health disparities, spurring a growing movement to challenge race essentialism and race-based medicine. The current research tested an intervention that educates college students about the historical construction of racial categories in the United States.
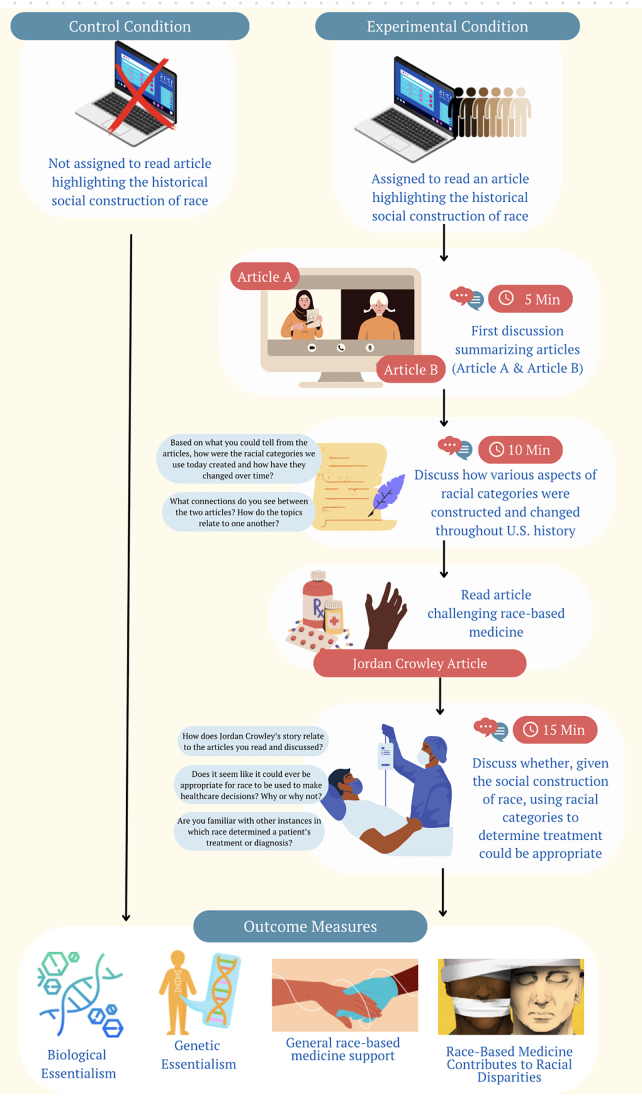
Methods: Participants who were randomly assigned to the intervention condition read an article highlighting the history of the sociopolitical construction of race. They were then prompted to discuss in dyads how racial categories were created and changed over history, and-in light of all this-the appropriateness of race-based medicine. Those assigned to the control condition advanced directly to the outcome measures.
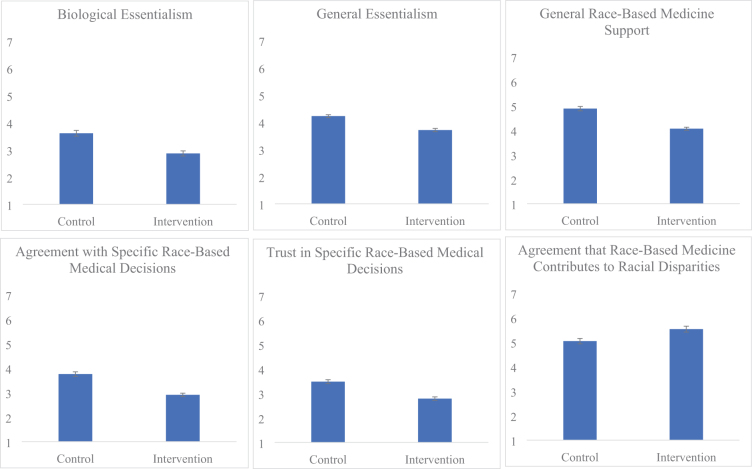
Results: Participants in the intervention condition reported less race essentialism, less support for race-based medicine, and greater belief that race-based medicine contributes to racial health disparities. Findings were not moderated by premed status.
Discussion: Our data provide initial evidence that our interactive intervention could effectively reduce biological essentialism and support for race-based medicine in both premed and non-premed students.
Health equity implications: This intervention has the potential to shape the way health care providers in-training understand race, their internalization of biologically essentialist explanations for disease, and willingness to adopt race-based treatment plans.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
