Hojin Yoon, Hanim Kwon, Sun-Uk Lee, Euyhyun Park, Chan-Nyoung Lee, Byung-Jo Kim, Ji-Soo Kim, Kun-Woo Park
{"title":"Scale for Ocular Motor Disorders in Ataxia (SODA) in Patients with Multiple System Atrophy","authors":"Hojin Yoon, Hanim Kwon, Sun-Uk Lee, Euyhyun Park, Chan-Nyoung Lee, Byung-Jo Kim, Ji-Soo Kim, Kun-Woo Park","doi":"10.1007/s12311-023-01653-y","DOIUrl":null,"url":null,"abstract":"<p>A clinical scale fully dedicated to evaluating ocular motor abnormalities is required for now. We investigated the utility of a recently developed Scale for Ocular motor Disorders in Ataxia (SODA) in patients with multiple system atrophy (MSA). We prospectively assessed SODA in consecutive patients with MSA between August 2021 and August 2023 at the Korea University Medical Center. The results of the clinical exam-based SODA were compared with those measured using video-oculography (VOG-guided SODA). We also compared the findings with other established clinical scales targeting patients with MSA, including the Unified Multiple System Atrophy Rating Scale (UMSARS) I-II, Movement Disorder Society-Unified Parkinson’s Disease Rating Scale motor part (UPDRS-III), Scale for Assessment of Rating of Ataxia (SARA), Composite Autonomic Symptom Score-31 (COMPASS-31), and Composite Autonomic Severity Score (CASS). Twenty patients were enrolled in our study (17 with cerebellar-type MSA and three with Parkinson-type MSA). Scores ranged from 1 to 14 (median [interquartile range (IQR)] = 8 [5−10]). Among the subscales, saccades had a median score of 2.5 (IQR = 1–3), followed by ocular pursuit (1 [0–1]), nystagmus (1 [0–2]), saccadic intrusions (1 [0–1]), vestibulo-ocular reflex (VOR) (0.5 [0–1]), ocular alignment (0 [0–1]), and VOR cancellation (1 [0–1]). The clinical-exam-based SODA (<i>p</i> = 0.020) and VOG-guided SODA (<i>p</i> = 0.034) positively correlated with disease duration. No correlation was found between clinical exam-based SODA and other scales. Skew deviation, gaze-evoked nystagmus, VOR cancellation, and smooth pursuit had the highest precision among the items. Ocular misalignment and spontaneous and positional nystagmus were frequently false positive and were poorly detected with clinical exam-based SODA. Six patients with repeated evaluation exhibited higher scores, along with deterioration documented on other clinical scales. The SODA can reliably predict neurodegeneration as an additional clinical surrogate in MSA.</p>","PeriodicalId":22415,"journal":{"name":"The Cerebellum","volume":"74 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-12-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Cerebellum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s12311-023-01653-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
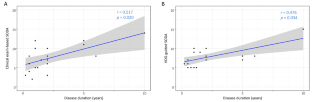
A clinical scale fully dedicated to evaluating ocular motor abnormalities is required for now. We investigated the utility of a recently developed Scale for Ocular motor Disorders in Ataxia (SODA) in patients with multiple system atrophy (MSA). We prospectively assessed SODA in consecutive patients with MSA between August 2021 and August 2023 at the Korea University Medical Center. The results of the clinical exam-based SODA were compared with those measured using video-oculography (VOG-guided SODA). We also compared the findings with other established clinical scales targeting patients with MSA, including the Unified Multiple System Atrophy Rating Scale (UMSARS) I-II, Movement Disorder Society-Unified Parkinson’s Disease Rating Scale motor part (UPDRS-III), Scale for Assessment of Rating of Ataxia (SARA), Composite Autonomic Symptom Score-31 (COMPASS-31), and Composite Autonomic Severity Score (CASS). Twenty patients were enrolled in our study (17 with cerebellar-type MSA and three with Parkinson-type MSA). Scores ranged from 1 to 14 (median [interquartile range (IQR)] = 8 [5−10]). Among the subscales, saccades had a median score of 2.5 (IQR = 1–3), followed by ocular pursuit (1 [0–1]), nystagmus (1 [0–2]), saccadic intrusions (1 [0–1]), vestibulo-ocular reflex (VOR) (0.5 [0–1]), ocular alignment (0 [0–1]), and VOR cancellation (1 [0–1]). The clinical-exam-based SODA (p = 0.020) and VOG-guided SODA (p = 0.034) positively correlated with disease duration. No correlation was found between clinical exam-based SODA and other scales. Skew deviation, gaze-evoked nystagmus, VOR cancellation, and smooth pursuit had the highest precision among the items. Ocular misalignment and spontaneous and positional nystagmus were frequently false positive and were poorly detected with clinical exam-based SODA. Six patients with repeated evaluation exhibited higher scores, along with deterioration documented on other clinical scales. The SODA can reliably predict neurodegeneration as an additional clinical surrogate in MSA.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
