{"title":"Effect of the Gupta Score on Pre-operative Cardiology Consultation Requests in Noncardiac Nonvascular Surgery.","authors":"Funda Atar, Fatma Özkan Sipahioğlu, Gülsen Keskin, Aslı Dönmez","doi":"10.4274/TJAR.2023.231464","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Cardiologists are the most frequently consulted specialists during pre-operative evaluations. However, unnecessary cardiology consultations (CC) can increase cardiologists' workload without impacting anaesthesia practice, resulting in delayed surgeries and additional financial burdens. We hypothesize that using Gupta during the preoperative period can reduce these adverse effects.</p><p><strong>Methods: </strong>This prospective study included patients scheduled for elective noncardiac, nonvascular surgeries who underwent pre-operative assessment. Patients who had no specific risk index used for preoperative cardiac risk evaluation were classified as Group I, and those evaluated using the Gupta scale were classified as Group II. The study compared preoperative CC, diagnostic tests, surgical delays, major adverse cardiac event (MACE), length of hospital stay and intensive care unit (ICU) stay, mortality, and costs.</p><p><strong>Results: </strong>A total of 898 patients were included in the study, with 487 in Group I and 411 in Group II. The Gupta group reduced the demand for preoperative CC (P<0.001) and preoperative non-invasive diagnostic testing (n = 107, 21.9% vs. n = 36, 8.75%). The time from the anaesthesiology outpatient clinic to surgery was 15 days in Group I and 14 days in Group II (<i>P</i>=0.132). The length of ICU stay was higher in Group I (<i>P</i>=0.019). MACE was 15 patients (3.08%) in Group I and 9 patients (2.19%) in Group II (<i>P</i>=0.076). The cost of patients in Group I was higher than that in Group II (<i>P</i>=0.019).</p><p><strong>Conclusion: </strong>Using Gupta in preoperative evaluation may reduce unnecessary preoperative resource usage, surgical delays, ICU hospitalization rates, additional costs, and mortality.</p>","PeriodicalId":23353,"journal":{"name":"Turkish journal of anaesthesiology and reanimation","volume":"51 6","pages":"485-490"},"PeriodicalIF":0.9000,"publicationDate":"2023-12-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10758665/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Turkish journal of anaesthesiology and reanimation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4274/TJAR.2023.231464","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Cardiologists are the most frequently consulted specialists during pre-operative evaluations. However, unnecessary cardiology consultations (CC) can increase cardiologists' workload without impacting anaesthesia practice, resulting in delayed surgeries and additional financial burdens. We hypothesize that using Gupta during the preoperative period can reduce these adverse effects.
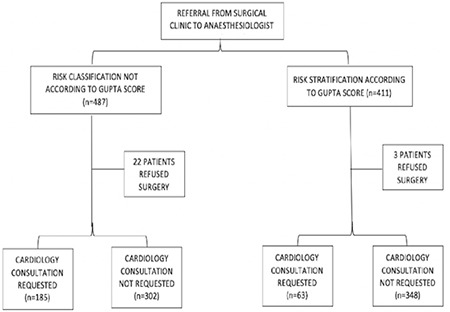
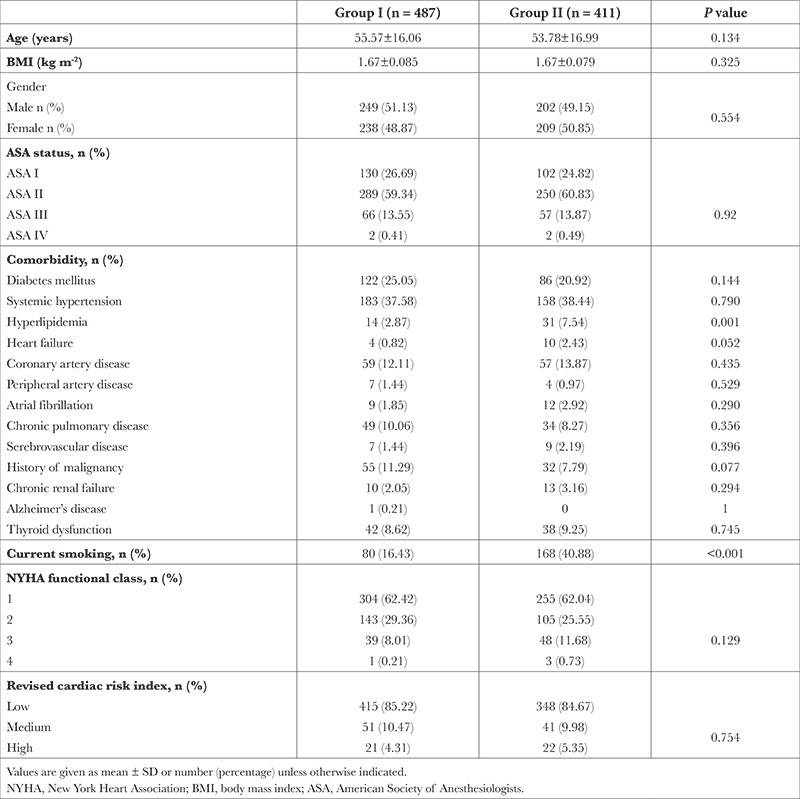
Methods: This prospective study included patients scheduled for elective noncardiac, nonvascular surgeries who underwent pre-operative assessment. Patients who had no specific risk index used for preoperative cardiac risk evaluation were classified as Group I, and those evaluated using the Gupta scale were classified as Group II. The study compared preoperative CC, diagnostic tests, surgical delays, major adverse cardiac event (MACE), length of hospital stay and intensive care unit (ICU) stay, mortality, and costs.
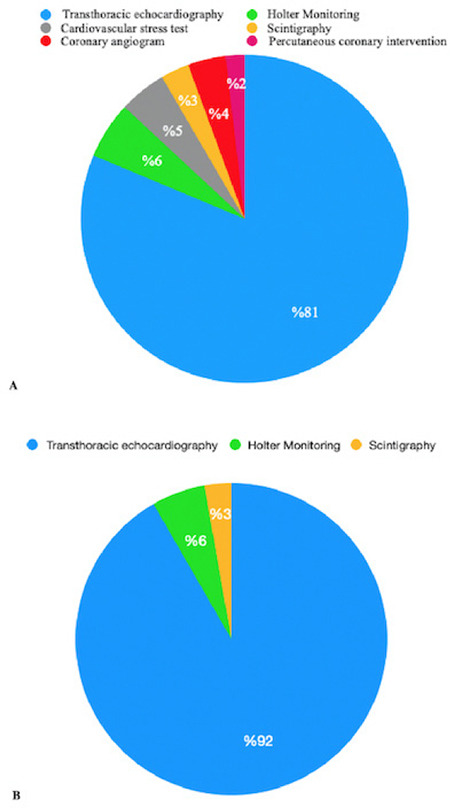
Results: A total of 898 patients were included in the study, with 487 in Group I and 411 in Group II. The Gupta group reduced the demand for preoperative CC (P<0.001) and preoperative non-invasive diagnostic testing (n = 107, 21.9% vs. n = 36, 8.75%). The time from the anaesthesiology outpatient clinic to surgery was 15 days in Group I and 14 days in Group II (P=0.132). The length of ICU stay was higher in Group I (P=0.019). MACE was 15 patients (3.08%) in Group I and 9 patients (2.19%) in Group II (P=0.076). The cost of patients in Group I was higher than that in Group II (P=0.019).
Conclusion: Using Gupta in preoperative evaluation may reduce unnecessary preoperative resource usage, surgical delays, ICU hospitalization rates, additional costs, and mortality.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
