Effect of prehospital advanced airway management on out-of-hospital cardiac arrest due to asphyxia: A JAAM-OHCA registry-based observational study in Japan
{"title":"Effect of prehospital advanced airway management on out-of-hospital cardiac arrest due to asphyxia: A JAAM-OHCA registry-based observational study in Japan","authors":"Naofumi Bunya, Ohnishi Hirofumi, Yutaka Igarashi, Tatsuya Norii, Yoichi Katayama, Takehiko Kasai, Keigo Sawamoto, Eichi Narimatsu","doi":"10.1002/ams2.912","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aim</h3>\n \n <p>To investigate the relationship between prehospital advanced airway management (AAM) and neurological outcomes in patients with asphyxia-related out-of-hospital cardiac arrest (OHCA).</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We retrospectively analyzed data from the Japanese Association for Acute Medicine OHCA registry between June 2014 and December 2017. Patients with asphyxia-related cardiac arrest aged ≥18 years were included. The primary outcome was a 1-month favorable neurological outcome (cerebral performance category [CPC] 1–2).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Of the 34,754 patients in the 2014–2017 JAAM-OHCA Registry, 1956 were included in our analysis. Cerebral performance category 1–2 was observed in 31 patients (1.6%), while CPC 3–5 was observed in 1925 patients (98.4%). Although prehospital AAM was associated with unfavorable neurological outcomes (odds ratio [OR], 0.269; 95% confidence interval [CI], 0.114–0.633; <i>p</i> = 0.003) in the univariate analysis, the association was not significant in the multivariate analysis. Compared with the AAM group, the non-AAM group showed increased rates of cardiac arrest after emergency medical service contact (4.3 vs. 7.2%, <i>p</i> = 0.009) and Glasgow Coma Scale ≥4 at hospital admission (1.9% vs. 4.7%, <i>p</i> = 0.004). Among the 903 patients for whom the time to return of spontaneous circulation (ROSC) could be calculated, the time from witnessed cardiac arrest to ROSC was significantly shorter (median, 8.5 vs. 37.0 min; <i>p</i> < 0.001) for those with favorable neurological outcomes than for those without.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Prehospital AAM is not associated with improved neurological outcomes among those with asphyxia-related OHCA. However, the time from cardiac arrest to the first ROSC was significantly shorter among those with favorable outcomes.</p>\n </section>\n </div>","PeriodicalId":7196,"journal":{"name":"Acute Medicine & Surgery","volume":"10 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2023-12-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ams2.912","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute Medicine & Surgery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ams2.912","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Aim
To investigate the relationship between prehospital advanced airway management (AAM) and neurological outcomes in patients with asphyxia-related out-of-hospital cardiac arrest (OHCA).
Methods
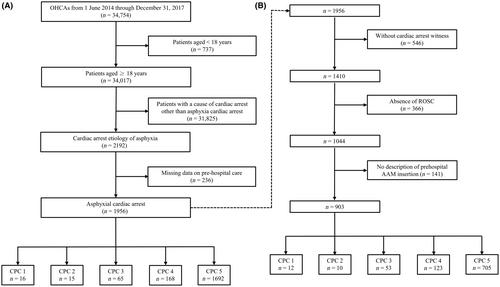
We retrospectively analyzed data from the Japanese Association for Acute Medicine OHCA registry between June 2014 and December 2017. Patients with asphyxia-related cardiac arrest aged ≥18 years were included. The primary outcome was a 1-month favorable neurological outcome (cerebral performance category [CPC] 1–2).
Results
Of the 34,754 patients in the 2014–2017 JAAM-OHCA Registry, 1956 were included in our analysis. Cerebral performance category 1–2 was observed in 31 patients (1.6%), while CPC 3–5 was observed in 1925 patients (98.4%). Although prehospital AAM was associated with unfavorable neurological outcomes (odds ratio [OR], 0.269; 95% confidence interval [CI], 0.114–0.633; p = 0.003) in the univariate analysis, the association was not significant in the multivariate analysis. Compared with the AAM group, the non-AAM group showed increased rates of cardiac arrest after emergency medical service contact (4.3 vs. 7.2%, p = 0.009) and Glasgow Coma Scale ≥4 at hospital admission (1.9% vs. 4.7%, p = 0.004). Among the 903 patients for whom the time to return of spontaneous circulation (ROSC) could be calculated, the time from witnessed cardiac arrest to ROSC was significantly shorter (median, 8.5 vs. 37.0 min; p < 0.001) for those with favorable neurological outcomes than for those without.
Conclusion
Prehospital AAM is not associated with improved neurological outcomes among those with asphyxia-related OHCA. However, the time from cardiac arrest to the first ROSC was significantly shorter among those with favorable outcomes.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
