Hamood Al Kindi, Hasina Al Harthi, Asim Al Balushi, Ahlam Atiq, Samiuddin Shaikh, Khalid Al Alawi, Abdullah Al-Farqani
{"title":"Blalock-Taussig Shunt versus Ductal Stenting as Palliation for Duct-Dependent Pulmonary Circulation.","authors":"Hamood Al Kindi, Hasina Al Harthi, Asim Al Balushi, Ahlam Atiq, Samiuddin Shaikh, Khalid Al Alawi, Abdullah Al-Farqani","doi":"10.18295/squmj.12.2023.073","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>There is limited data published from outside North America and Europe comparing the outcomes of a modified Blalock-Taussig shunt (MBTS) and ductal stenting as the first palliative procedure for infants with duct-dependent pulmonary circulation. This study reports the National Heart Center's, in Muscat, Oman, experience in comparing the outcomes of these 2 interventions.</p><p><strong>Methods: </strong>This retrospective study included all infants with duct-dependent pulmonary circulation who received either a MBTS or ductal stenting from 2016-2019. The primary outcomes were death or re-interventions. Secondary outcomes included death, subsequent re-interventions, survival to subsequent surgical intervention, survival to hospital discharge, post-procedural mechanical ventilation and duration of intensive care unit stay.</p><p><strong>Results: </strong>A total of 71 patients were included in the study, 33 (46%) of whom received ductal stenting. The prevalence of the primary outcome (death or re-intervention) in the patent ductus arteriosus (PDA) stent group was 54.5% versus 31.6% in the MBTS group but this was not statistically significant (<i>P</i> = 0.06). There was no difference between the 2 groups in terms of time to next surgical intervention (<i>P</i> = 0.233). The PDA stent group had shorter post-procedural, mechanical ventilation and intensive care unit stay durations (<i>P</i> <0.05). Syndromic patients were at higher risk of mortality compared to non-syndromic patients.</p><p><strong>Conclusion: </strong>MBTS and ductal stenting are both acceptable modalities as a palliative intervention for infants with duct-dependant pulmonary circulation. Syndromic patients are at higher risk of mortality. This can be considered an important factor for patient selection.</p>","PeriodicalId":22083,"journal":{"name":"Sultan Qaboos University Medical Journal","volume":"23 Spec Iss","pages":"10-15"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10754312/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Sultan Qaboos University Medical Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18295/squmj.12.2023.073","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: There is limited data published from outside North America and Europe comparing the outcomes of a modified Blalock-Taussig shunt (MBTS) and ductal stenting as the first palliative procedure for infants with duct-dependent pulmonary circulation. This study reports the National Heart Center's, in Muscat, Oman, experience in comparing the outcomes of these 2 interventions.
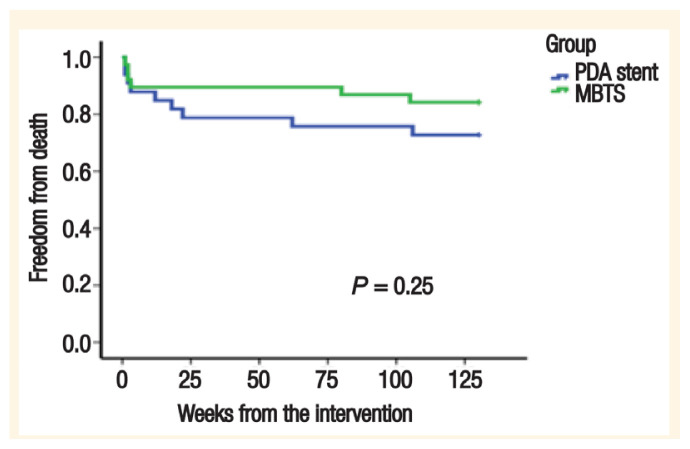
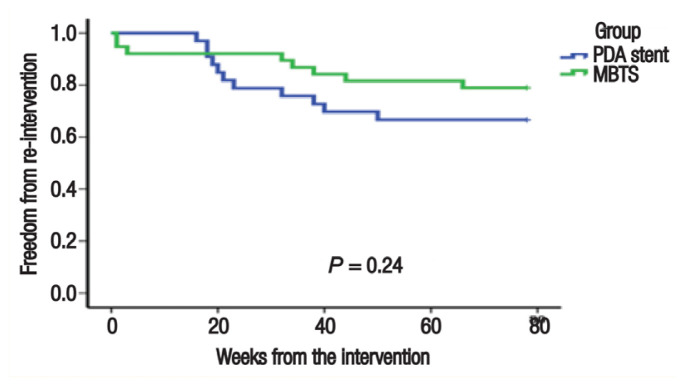
Methods: This retrospective study included all infants with duct-dependent pulmonary circulation who received either a MBTS or ductal stenting from 2016-2019. The primary outcomes were death or re-interventions. Secondary outcomes included death, subsequent re-interventions, survival to subsequent surgical intervention, survival to hospital discharge, post-procedural mechanical ventilation and duration of intensive care unit stay.
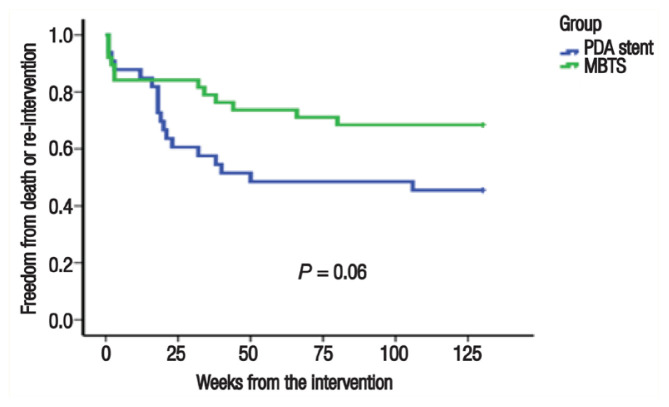
Results: A total of 71 patients were included in the study, 33 (46%) of whom received ductal stenting. The prevalence of the primary outcome (death or re-intervention) in the patent ductus arteriosus (PDA) stent group was 54.5% versus 31.6% in the MBTS group but this was not statistically significant (P = 0.06). There was no difference between the 2 groups in terms of time to next surgical intervention (P = 0.233). The PDA stent group had shorter post-procedural, mechanical ventilation and intensive care unit stay durations (P <0.05). Syndromic patients were at higher risk of mortality compared to non-syndromic patients.
Conclusion: MBTS and ductal stenting are both acceptable modalities as a palliative intervention for infants with duct-dependant pulmonary circulation. Syndromic patients are at higher risk of mortality. This can be considered an important factor for patient selection.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
