Ofir Deri, David Ovadia, Ella Huszti, Michael Peled, Milton Saute, Tammy Hod, Amir Onn, Lior Seluk, Nadav Furie, Inbal Shafran, Ronen Mass, Sumit Chatterji, Liran Levy
{"title":"Referral rates and barriers to lung transplantation based on pulmonary function criteria in interstitial lung diseases: a retrospective cohort study.","authors":"Ofir Deri, David Ovadia, Ella Huszti, Michael Peled, Milton Saute, Tammy Hod, Amir Onn, Lior Seluk, Nadav Furie, Inbal Shafran, Ronen Mass, Sumit Chatterji, Liran Levy","doi":"10.1177/17534666231221750","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Interstitial lung diseases (ILD) unresponsive to medical therapy often require lung transplantation (LTx), which prolongs quality of life and survival. Ideal timing for referral for LTx remains challenging, with late referral associated with significant morbidity and mortality. Among other criteria, patients with ILD should be considered for LTx if forced vital capacity (FVC) is less than 80% or diffusion capacity for carbon monoxide (DLCO) is less than 40%. However, data on referral rates are lacking.</p><p><strong>Objectives: </strong>To evaluate referral rates for LTx based on pulmonary function tests (PFTs) and identify barriers associated with non-referral.</p><p><strong>Design: </strong>A single-center retrospective cohort study.</p><p><strong>Methods: </strong>The study consisted of ILD patients who performed PFT between 2014 and 2020. Patients with FVC < 80% or a DLCO < 40% were included in the study. Patients with absolute contraindications to LTx were excluded. Referral rates were computed, and a comparison was made between referred and non-referred subjects.</p><p><strong>Results: </strong>Out of 114 ILD patients meeting criteria for referral to LTx, 35 were referred (30.7%), and 7 proceeded to undergo LTx. Median time from PFT to referral for assessment was 255 days [interquartile range (IQR) 35-1077]. Median time from referral to LTx was 89 days (IQR 59-143). Referred patients were younger (<i>p</i> = 0.003), had lower FVC (<i>p</i> < 0.001), DLCO (<i>p</i> < 0.001), and a higher rate of pulmonary hypertension (<i>p</i> = 0.04). Relatively better PFT, and older age, were significantly associated with non-referral of patients.</p><p><strong>Conclusion: </strong>There is under-referral of ILD patients who are eligible for LTx, which is associated with severe disease and missed opportunities for LTx. Further research is required to validate these findings.</p>","PeriodicalId":22884,"journal":{"name":"Therapeutic Advances in Respiratory Disease","volume":"18 ","pages":"17534666231221750"},"PeriodicalIF":3.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10771041/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Respiratory Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17534666231221750","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Interstitial lung diseases (ILD) unresponsive to medical therapy often require lung transplantation (LTx), which prolongs quality of life and survival. Ideal timing for referral for LTx remains challenging, with late referral associated with significant morbidity and mortality. Among other criteria, patients with ILD should be considered for LTx if forced vital capacity (FVC) is less than 80% or diffusion capacity for carbon monoxide (DLCO) is less than 40%. However, data on referral rates are lacking.
Objectives: To evaluate referral rates for LTx based on pulmonary function tests (PFTs) and identify barriers associated with non-referral.
Design: A single-center retrospective cohort study.
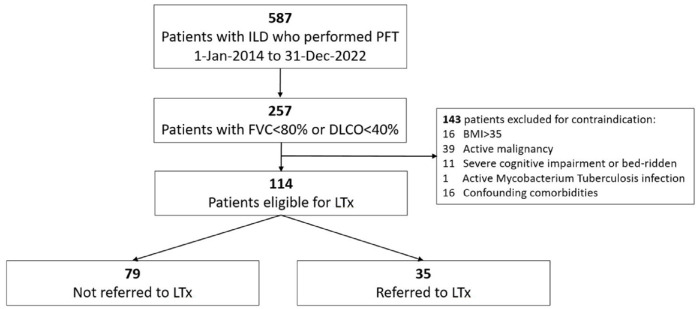
Methods: The study consisted of ILD patients who performed PFT between 2014 and 2020. Patients with FVC < 80% or a DLCO < 40% were included in the study. Patients with absolute contraindications to LTx were excluded. Referral rates were computed, and a comparison was made between referred and non-referred subjects.
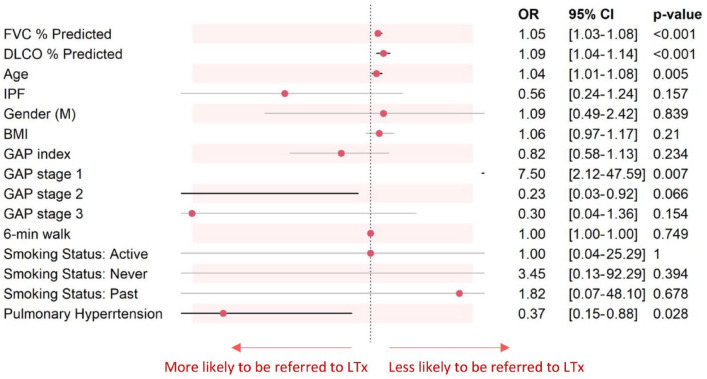
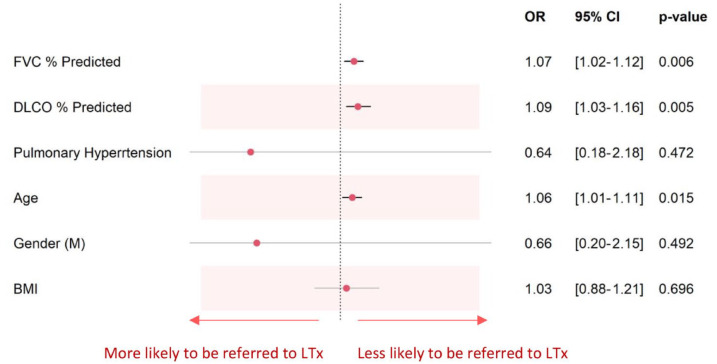
Results: Out of 114 ILD patients meeting criteria for referral to LTx, 35 were referred (30.7%), and 7 proceeded to undergo LTx. Median time from PFT to referral for assessment was 255 days [interquartile range (IQR) 35-1077]. Median time from referral to LTx was 89 days (IQR 59-143). Referred patients were younger (p = 0.003), had lower FVC (p < 0.001), DLCO (p < 0.001), and a higher rate of pulmonary hypertension (p = 0.04). Relatively better PFT, and older age, were significantly associated with non-referral of patients.
Conclusion: There is under-referral of ILD patients who are eligible for LTx, which is associated with severe disease and missed opportunities for LTx. Further research is required to validate these findings.
期刊介绍:
Therapeutic Advances in Respiratory Disease delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of respiratory disease.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
