{"title":"Blood flow ratio in the gastric conduit measured by laser Doppler flowmetry: A predictor of anastomotic leakage after esophagectomy","authors":"Hirotaka Ishida, Toshiaki Fukutomi, Yusuke Taniyama, Chiaki Sato, Hiroshi Okamoto, Yohei Ozawa, Yu Onodera, Ken Koseki, Michiaki Unno, Takashi Kamei","doi":"10.1002/ags3.12754","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Anastomotic leakage after esophagectomy is a common complication. Laser Doppler flowmetry (LDF) can quantitatively evaluate the blood flow in the gastric conduit.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A total of 326 patients who underwent thoracoscopic/robot-assisted esophagectomy followed by gastric conduit reconstruction and end-to-side anastomosis were enrolled. We divided the gastric conduit into zones I (dominated by the right gastroepiploic vessels), II (dominated by the left gastroepiploic vessels), and III (perfused with short gastric vessels). Before pulling up the gastric conduit to the neck, LDF values were measured at the pylorus, the border between zones I and II (zone I/II), the border between zones II and III (zone II/III), and the gastric conduit tip (tip). The blood flow ratio was calculated as the LDF value divided by the LDF value at the pylorus.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Anastomotic leakage developed in 32 of 326 patients. Leakage was significantly associated with the blood flow ratio at the tip (<i>p</i> < 0.001), but not at zone I/II, zone II/III, and the anastomotic site. The receiver-operating characteristic curve analysis identified an anastomotic leakage cutoff ratio of 0.41 (at the tip). A multivariate Cox analysis showed that a blood flow ratio <0.41 at the tip was an independent risk factor for anastomotic leakage (<i>p</i> < 0.001).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Anastomotic leakage after esophagectomy was significantly associated with the blood flow ratio at the tip of the gastric conduit. Preservation of the blood supply to the tip via the gastric wall might contribute to a decreased incidence of anastomotic leakage.</p>\n </section>\n </div>","PeriodicalId":8030,"journal":{"name":"Annals of Gastroenterological Surgery","volume":"8 2","pages":"234-242"},"PeriodicalIF":3.3000,"publicationDate":"2023-11-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ags3.12754","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterological Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12754","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Anastomotic leakage after esophagectomy is a common complication. Laser Doppler flowmetry (LDF) can quantitatively evaluate the blood flow in the gastric conduit.
Methods
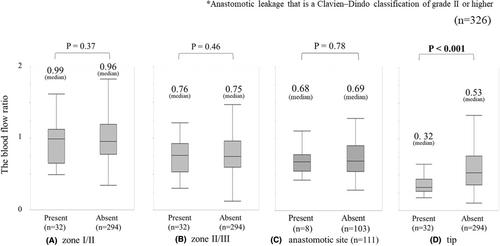
A total of 326 patients who underwent thoracoscopic/robot-assisted esophagectomy followed by gastric conduit reconstruction and end-to-side anastomosis were enrolled. We divided the gastric conduit into zones I (dominated by the right gastroepiploic vessels), II (dominated by the left gastroepiploic vessels), and III (perfused with short gastric vessels). Before pulling up the gastric conduit to the neck, LDF values were measured at the pylorus, the border between zones I and II (zone I/II), the border between zones II and III (zone II/III), and the gastric conduit tip (tip). The blood flow ratio was calculated as the LDF value divided by the LDF value at the pylorus.
Results
Anastomotic leakage developed in 32 of 326 patients. Leakage was significantly associated with the blood flow ratio at the tip (p < 0.001), but not at zone I/II, zone II/III, and the anastomotic site. The receiver-operating characteristic curve analysis identified an anastomotic leakage cutoff ratio of 0.41 (at the tip). A multivariate Cox analysis showed that a blood flow ratio <0.41 at the tip was an independent risk factor for anastomotic leakage (p < 0.001).
Conclusion
Anastomotic leakage after esophagectomy was significantly associated with the blood flow ratio at the tip of the gastric conduit. Preservation of the blood supply to the tip via the gastric wall might contribute to a decreased incidence of anastomotic leakage.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
