Jorge Jorquera, Jorge Dreyse, Constanza Salas, Francisca Letelier, Bunio Weissglas, Javiera Del-Río, Mario Henríquez-Beltrán, Gonzalo Labarca, Jorge Jorquera-Díaz
{"title":"Clinical Application of the Multicomponent Grading System for Sleep Apnea Classification and Incident Cardiovascular Mortality.","authors":"Jorge Jorquera, Jorge Dreyse, Constanza Salas, Francisca Letelier, Bunio Weissglas, Javiera Del-Río, Mario Henríquez-Beltrán, Gonzalo Labarca, Jorge Jorquera-Díaz","doi":"10.1055/s-0043-1776770","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objective</b> To evaluate the clinical utility of the Baveno classification in predicting incident cardiovascular mortality after five years of follow-up in a clinic-based cohort of patients with obstructive sleep apnea (OSA). <b>Materials and Methods</b> We evaluated the reproducibility of the Baveno classification using data from the Santiago Obstructive Sleep Apnea (SantOSA) study. The groups were labeled Baveno A (minor symptoms and comorbidities), B (severe symptoms and minor comorbidities), C (minor symptoms and severe comorbidities), and D (severe symptoms and comorbidities). Within-group comparisons were performed using analysis of variance (ANOVA) and post hoc tests. The associations between groups and incident cardiovascular mortality were determined through the Mantel-Cox and Cox proportional hazard ratios (HRs) adjusted by covariables. <b>Results</b> A total of 1,300 OSA patients were included (Baveno A: 27.7%; B: 28%; C: 16.8%; and D: 27.5%). The follow-up was of 5.4 years. Compared to Baveno A, the fully-adjusted risk of cardiovascular mortality with Baveno B presented an HR of 1.38 (95% confidence interval [95%CI]: 0.14-13.5; <i>p</i> = 0.78); with Baveno C, it was of 1.71 (95%CI: 0.18-16.2; <i>p</i> = 0.63); and, with Baveno D, of 1.04 (95%CI: 0.12-9.2; <i>p</i> = 0.98). We found no interactions involving Baveno group, sex and OSA severity. <b>Discussion</b> Among OSA patients, the Baveno classification can describe different subgroups. However, its utility in identifying incident cardiovascular mortality is unclear. Long-term follow-up studies and the inclusion of demographic variables in the classification could improve its ability to detect a high-risk phenotype associated with cardiovascular mortality. <b>Conclusion</b> The Baveno classification serves as a valuable method for categorizing varying groups of patients afflicted with OSA. Nevertheless, its precision in identifying occurrence of cardiovascular mortality is still unclear.</p>","PeriodicalId":21848,"journal":{"name":"Sleep Science","volume":"16 4","pages":"e446-e453"},"PeriodicalIF":1.8000,"publicationDate":"2023-11-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10773515/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Sleep Science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0043-1776770","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
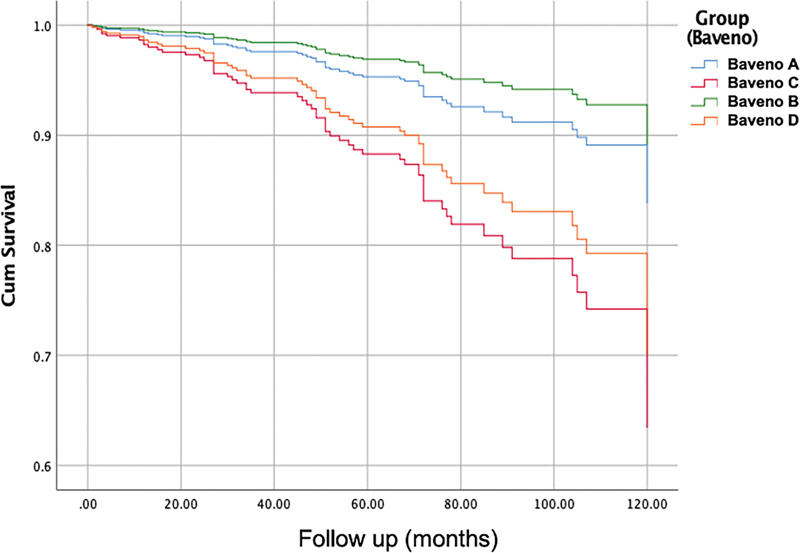
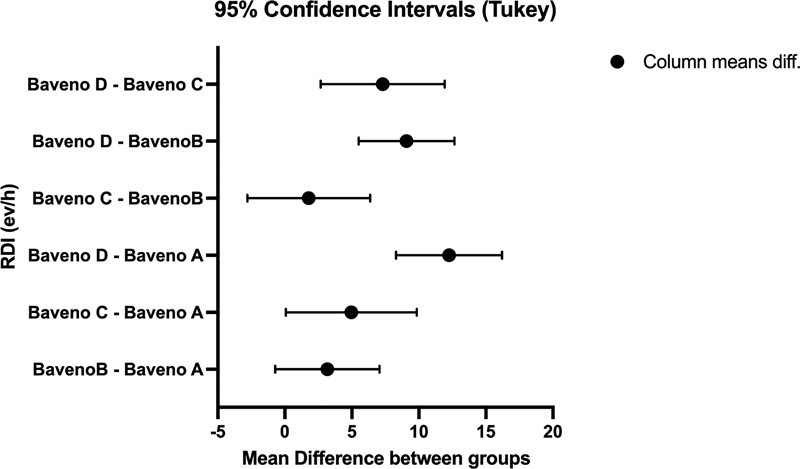
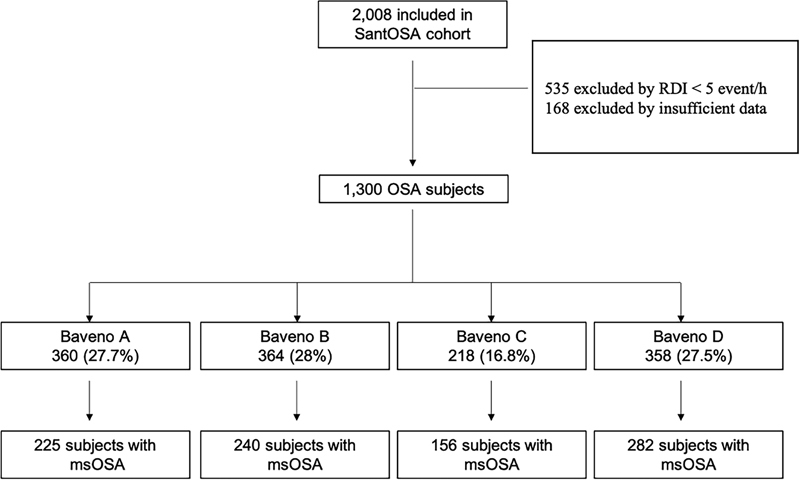
Objective To evaluate the clinical utility of the Baveno classification in predicting incident cardiovascular mortality after five years of follow-up in a clinic-based cohort of patients with obstructive sleep apnea (OSA). Materials and Methods We evaluated the reproducibility of the Baveno classification using data from the Santiago Obstructive Sleep Apnea (SantOSA) study. The groups were labeled Baveno A (minor symptoms and comorbidities), B (severe symptoms and minor comorbidities), C (minor symptoms and severe comorbidities), and D (severe symptoms and comorbidities). Within-group comparisons were performed using analysis of variance (ANOVA) and post hoc tests. The associations between groups and incident cardiovascular mortality were determined through the Mantel-Cox and Cox proportional hazard ratios (HRs) adjusted by covariables. Results A total of 1,300 OSA patients were included (Baveno A: 27.7%; B: 28%; C: 16.8%; and D: 27.5%). The follow-up was of 5.4 years. Compared to Baveno A, the fully-adjusted risk of cardiovascular mortality with Baveno B presented an HR of 1.38 (95% confidence interval [95%CI]: 0.14-13.5; p = 0.78); with Baveno C, it was of 1.71 (95%CI: 0.18-16.2; p = 0.63); and, with Baveno D, of 1.04 (95%CI: 0.12-9.2; p = 0.98). We found no interactions involving Baveno group, sex and OSA severity. Discussion Among OSA patients, the Baveno classification can describe different subgroups. However, its utility in identifying incident cardiovascular mortality is unclear. Long-term follow-up studies and the inclusion of demographic variables in the classification could improve its ability to detect a high-risk phenotype associated with cardiovascular mortality. Conclusion The Baveno classification serves as a valuable method for categorizing varying groups of patients afflicted with OSA. Nevertheless, its precision in identifying occurrence of cardiovascular mortality is still unclear.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
