Ashley Deutsch, Kye Poroksy, Lauren Westafer, Paul Visintainer, Timothy Mader
{"title":"Validity of Computer-interpreted \"Normal\" and \"Otherwise Normal\" ECG in Emergency Department Triage Patients.","authors":"Ashley Deutsch, Kye Poroksy, Lauren Westafer, Paul Visintainer, Timothy Mader","doi":"10.5811/westjem.58464","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Chest pain is the second most common chief complaint for patients undergoing evaluation in emergency departments (ED) in the United States. The American Heart Association recommends immediate physician interpretation of all electrocardiograms (ECG) performed for adults with chest pain within 10 minutes to evaluate for the finding of ST-elevation myocardial infarction (STEMI). The ECG machines provide computerized interpretation of each ECG, potentially obviating the need for immediate physician analysis; however, the reliability of computer-interpreted findings of \"normal\" or \"otherwise normal\" ECG to rule out STEMI requiring immediate intervention in the ED is unknown.</p><p><strong>Methods: </strong>We performed a prospective cohort analysis of 2,275 ECGs performed in triage in the adult ED of a single academic medical center, comparing the computerized interpretations of \"normal\" and \"otherwise normal\" ECGs to those of attending cardiologists. ECGs were obtained with a GE MAC 5500 machine and interpreted using Marquette 12SL.</p><p><strong>Results: </strong>In our study population, a triage ECG with a computerized interpretation of \"normal\" or \"otherwise normal\" ECG had a negative predictive value of 100% for STEMI (one-sided, lower 97.5% confidence interval 99.6%). None of the studied patients with these ECG interpretations had a final diagnosis of STEMI, acute coronary syndrome, or other diagnosis requiring emergent cardiac catheterization.</p><p><strong>Conclusion: </strong>In our study population, ECG machine interpretations of \"normal\" or \"otherwise normal\" ECG excluded findings of STEMI. The ECGs with these computerized interpretations could safely wait for physician interpretation until the time of patient evaluation without delaying an acute STEMI diagnosis.</p>","PeriodicalId":23682,"journal":{"name":"Western Journal of Emergency Medicine","volume":"25 1","pages":"3-8"},"PeriodicalIF":2.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10777178/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Western Journal of Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5811/westjem.58464","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Chest pain is the second most common chief complaint for patients undergoing evaluation in emergency departments (ED) in the United States. The American Heart Association recommends immediate physician interpretation of all electrocardiograms (ECG) performed for adults with chest pain within 10 minutes to evaluate for the finding of ST-elevation myocardial infarction (STEMI). The ECG machines provide computerized interpretation of each ECG, potentially obviating the need for immediate physician analysis; however, the reliability of computer-interpreted findings of "normal" or "otherwise normal" ECG to rule out STEMI requiring immediate intervention in the ED is unknown.
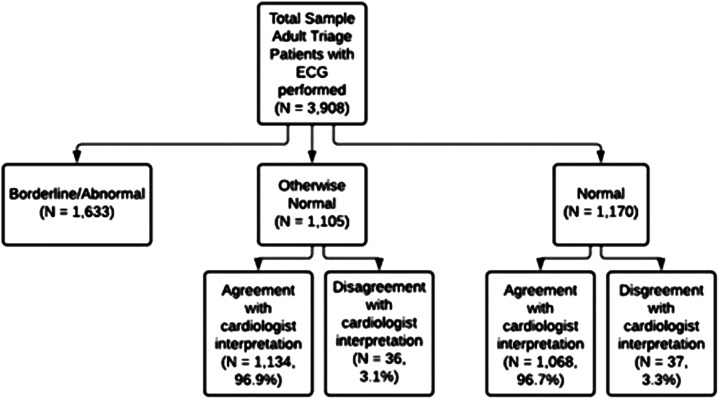
Methods: We performed a prospective cohort analysis of 2,275 ECGs performed in triage in the adult ED of a single academic medical center, comparing the computerized interpretations of "normal" and "otherwise normal" ECGs to those of attending cardiologists. ECGs were obtained with a GE MAC 5500 machine and interpreted using Marquette 12SL.
Results: In our study population, a triage ECG with a computerized interpretation of "normal" or "otherwise normal" ECG had a negative predictive value of 100% for STEMI (one-sided, lower 97.5% confidence interval 99.6%). None of the studied patients with these ECG interpretations had a final diagnosis of STEMI, acute coronary syndrome, or other diagnosis requiring emergent cardiac catheterization.
Conclusion: In our study population, ECG machine interpretations of "normal" or "otherwise normal" ECG excluded findings of STEMI. The ECGs with these computerized interpretations could safely wait for physician interpretation until the time of patient evaluation without delaying an acute STEMI diagnosis.
期刊介绍:
WestJEM focuses on how the systems and delivery of emergency care affects health, health disparities, and health outcomes in communities and populations worldwide, including the impact of social conditions on the composition of patients seeking care in emergency departments.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
