Perioperative copeptin: predictive value and risk stratification in patients undergoing major noncardiac surgery-a prospective observational cohort study.
Firmin Kamber, Sebastian Roth, Daniel Bolliger, Esther Seeberger, Johannes Nienhaus, Christian Mueller, Giovanna Lurati Buse, Eckhard Mauermann
{"title":"Perioperative copeptin: predictive value and risk stratification in patients undergoing major noncardiac surgery-a prospective observational cohort study.","authors":"Firmin Kamber, Sebastian Roth, Daniel Bolliger, Esther Seeberger, Johannes Nienhaus, Christian Mueller, Giovanna Lurati Buse, Eckhard Mauermann","doi":"10.1007/s12630-023-02677-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Biomarkers can aid in perioperative risk stratification. While preoperative copeptin has been associated with adverse events, intraoperative information is lacking and this association may rather reflect a baseline risk. Knowledge about correlations between postoperative copeptin measurements and clinically relevant outcomes is scarce. We examined the association of perioperative copeptin concentrations with postoperative all-cause mortality and/or major adverse cardiac and cerebrovascular events (MACCE) at 12 months and 30 days as well as with perioperative myocardial injury (PMI).</p><p><strong>Methods: </strong>We conducted a prospective observational cohort study of adults undergoing noncardiac surgery with intermediate to high surgical risk in Basel, Switzerland, and Düsseldorf, Germany from February 2016 to December 2020. We measured copeptin and cardiac troponin before surgery, immediately after surgery (0 hr) and once between the second and fourth postoperative day (POD 2-4).</p><p><strong>Results: </strong>A primary outcome event of a composite of all-cause mortality and/or MACCE at 12 months occurred in 48/502 patients (9.6%). Elevated preoperative copeptin (> 14 pmol·L<sup>-1</sup>), immediate postoperative copeptin (> 90 pmol·L<sup>-1</sup>), and copeptin on POD 2-4 (> 14 pmol·L<sup>-1</sup>) were associated with lower one-year MACCE-free and/or mortality-free survival (hazard ratio [HR], 2.89; 95% confidence interval [CI], 1.62 to 5.2; HR, 2.07; 95% CI, 1.17 to 3.66; and HR, 2.47; 95% CI, 1.36 to 4.46, respectively). Multivariable analysis continued to show an association for preoperative and postoperative copeptin on POD 2-4. Furthermore, elevated copeptin on POD 2-4 showed an association with 30-day MACCE-free survival (HR, 2.15; 95% CI, 1.18 to 3.91). A total of 64 of 489 patients showed PMI (13.1%). Elevated preoperative copeptin was not associated with PMI, while immediate postoperative copeptin was modestly associated with PMI.</p><p><strong>Conclusion: </strong>The results of the present prospective observational cohort study suggest that perioperative copeptin concentrations can help identify patients at risk for all-cause mortality and/or MACCE. Other identified risk factors were revised cardiac risk index, body mass index, surgical risk, and preoperative hemoglobin.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov (NCT02687776); first submitted 9 February 2016.</p>","PeriodicalId":56145,"journal":{"name":"Canadian Journal of Anesthesia-Journal Canadien D Anesthesie","volume":" ","pages":"330-342"},"PeriodicalIF":3.3000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10923994/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Anesthesia-Journal Canadien D Anesthesie","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12630-023-02677-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/19 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Biomarkers can aid in perioperative risk stratification. While preoperative copeptin has been associated with adverse events, intraoperative information is lacking and this association may rather reflect a baseline risk. Knowledge about correlations between postoperative copeptin measurements and clinically relevant outcomes is scarce. We examined the association of perioperative copeptin concentrations with postoperative all-cause mortality and/or major adverse cardiac and cerebrovascular events (MACCE) at 12 months and 30 days as well as with perioperative myocardial injury (PMI).
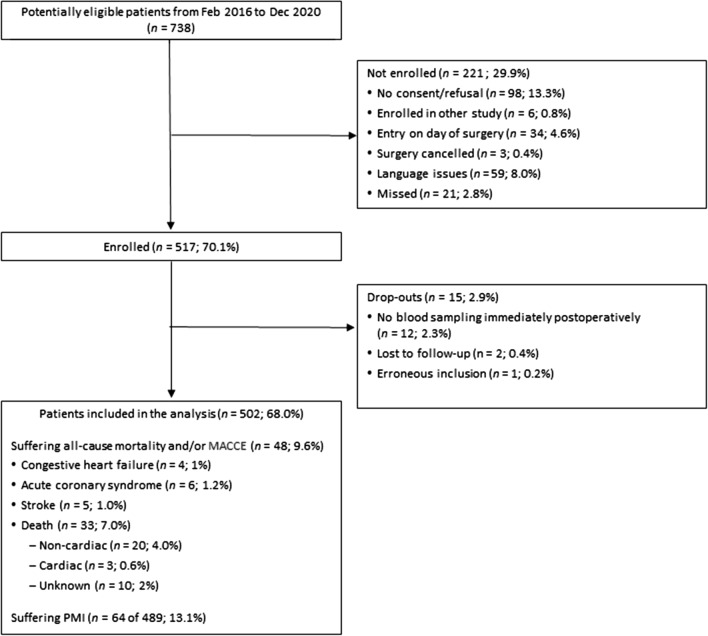
Methods: We conducted a prospective observational cohort study of adults undergoing noncardiac surgery with intermediate to high surgical risk in Basel, Switzerland, and Düsseldorf, Germany from February 2016 to December 2020. We measured copeptin and cardiac troponin before surgery, immediately after surgery (0 hr) and once between the second and fourth postoperative day (POD 2-4).
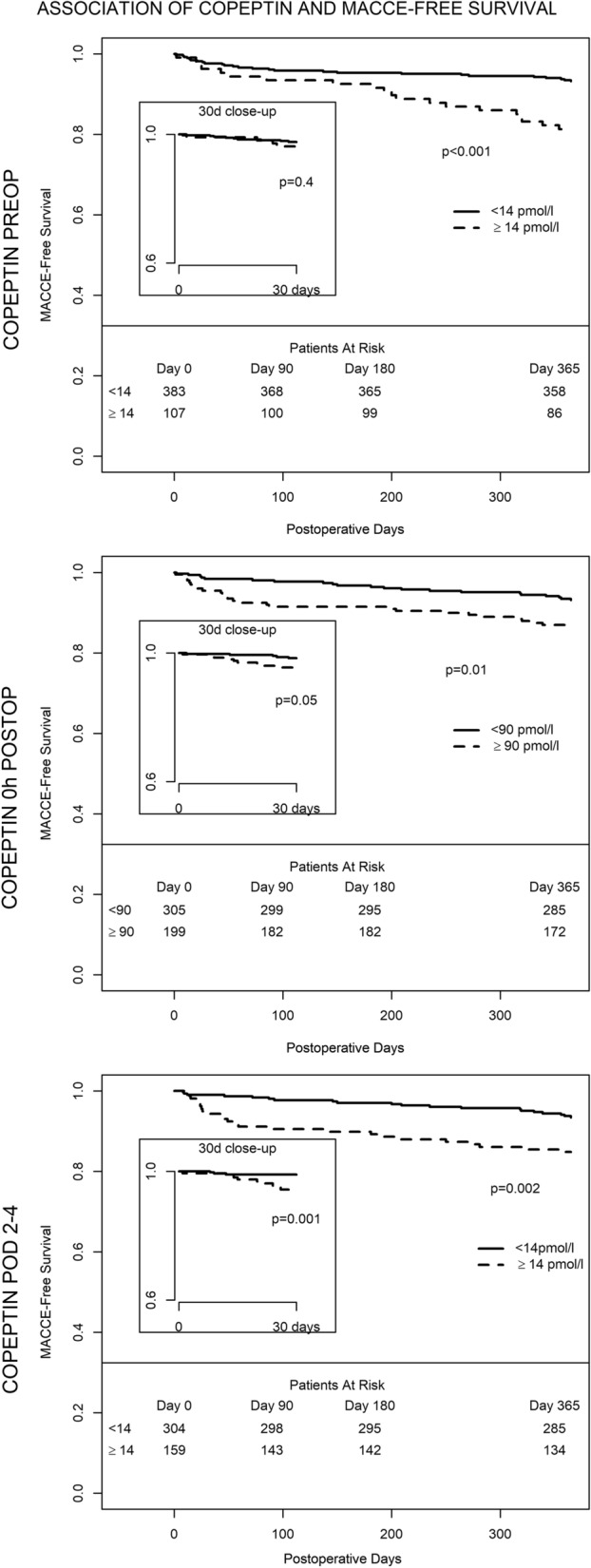
Results: A primary outcome event of a composite of all-cause mortality and/or MACCE at 12 months occurred in 48/502 patients (9.6%). Elevated preoperative copeptin (> 14 pmol·L-1), immediate postoperative copeptin (> 90 pmol·L-1), and copeptin on POD 2-4 (> 14 pmol·L-1) were associated with lower one-year MACCE-free and/or mortality-free survival (hazard ratio [HR], 2.89; 95% confidence interval [CI], 1.62 to 5.2; HR, 2.07; 95% CI, 1.17 to 3.66; and HR, 2.47; 95% CI, 1.36 to 4.46, respectively). Multivariable analysis continued to show an association for preoperative and postoperative copeptin on POD 2-4. Furthermore, elevated copeptin on POD 2-4 showed an association with 30-day MACCE-free survival (HR, 2.15; 95% CI, 1.18 to 3.91). A total of 64 of 489 patients showed PMI (13.1%). Elevated preoperative copeptin was not associated with PMI, while immediate postoperative copeptin was modestly associated with PMI.
Conclusion: The results of the present prospective observational cohort study suggest that perioperative copeptin concentrations can help identify patients at risk for all-cause mortality and/or MACCE. Other identified risk factors were revised cardiac risk index, body mass index, surgical risk, and preoperative hemoglobin.
Trial registration: ClinicalTrials.gov (NCT02687776); first submitted 9 February 2016.
期刊介绍:
The Canadian Journal of Anesthesia (the Journal) is owned by the Canadian Anesthesiologists’
Society and is published by Springer Science + Business Media, LLM (New York). From the
first year of publication in 1954, the international exposure of the Journal has broadened
considerably, with articles now received from over 50 countries. The Journal is published
monthly, and has an impact Factor (mean journal citation frequency) of 2.127 (in 2012). Article
types consist of invited editorials, reports of original investigations (clinical and basic sciences
articles), case reports/case series, review articles, systematic reviews, accredited continuing
professional development (CPD) modules, and Letters to the Editor. The editorial content,
according to the mission statement, spans the fields of anesthesia, acute and chronic pain,
perioperative medicine and critical care. In addition, the Journal publishes practice guidelines
and standards articles relevant to clinicians. Articles are published either in English or in French,
according to the language of submission.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
