Muhammad A. Zafar, Andrew F. Beck, Chris Chirumbolo, Ken D. Wilson, Kate Haralson, Katherine Rich, Peter Margolis, David Hartley
{"title":"A regional learning health system of congregate care facilities for COVID-19 response","authors":"Muhammad A. Zafar, Andrew F. Beck, Chris Chirumbolo, Ken D. Wilson, Kate Haralson, Katherine Rich, Peter Margolis, David Hartley","doi":"10.1002/lrh2.10407","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>The COVID-19 pandemic disproportionately affected congregate care (CC) facilities due to communal living, presence of vulnerable populations, inadequate preventive resources, and limited ability to respond to the pandemic's rapidly evolving phases. Most facilities function independently and are not organized for collaborative learning and operations.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We formed a learning health system of CC facilities in our 14-county metropolitan region, coordinated with public health and health care sectors, to address challenges driven by COVID-19. A CC steering committee (SC) was formed that represented diverse institutions and viewpoints, including skilled nursing facilities, transitional care facilities, residential facilities, prisons, and shelters. The SC met regularly and was guided by situational awareness and systems thinking. A regional CC COVID-19 dashboard was developed based on publicly available data and weekly data submitted by participating facilities. Those experiencing outbreaks or supply shortages were quickly identified. As the pandemic progressed, the role of the SC shifted to address new and forecasted needs.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Over 60 facilities participated in data sharing. The SC shared new guidelines, regulations, educational material, and best practices with the participating facilities. Information about testing sites, supplies, vaccination rollout, and facilities that had the capacity to accept COVID-19 patients was regularly disseminated. The SC was able to direct resources to those facilities experiencing outbreaks or supply shortages.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>A novel learning health system of regional CC facilities enabled preparedness, situational awareness, collaboration, and rapid dissemination of best practices across pandemic phases. Such collaborative efforts can play an important role in addressing other public and preventive health challenges.</p>\n </section>\n </div>","PeriodicalId":43916,"journal":{"name":"Learning Health Systems","volume":"8 3","pages":""},"PeriodicalIF":2.6000,"publicationDate":"2024-01-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lrh2.10407","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Learning Health Systems","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/lrh2.10407","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction
The COVID-19 pandemic disproportionately affected congregate care (CC) facilities due to communal living, presence of vulnerable populations, inadequate preventive resources, and limited ability to respond to the pandemic's rapidly evolving phases. Most facilities function independently and are not organized for collaborative learning and operations.
Methods
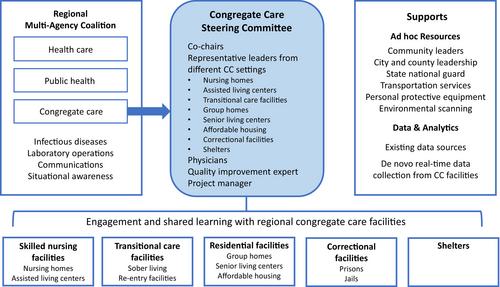
We formed a learning health system of CC facilities in our 14-county metropolitan region, coordinated with public health and health care sectors, to address challenges driven by COVID-19. A CC steering committee (SC) was formed that represented diverse institutions and viewpoints, including skilled nursing facilities, transitional care facilities, residential facilities, prisons, and shelters. The SC met regularly and was guided by situational awareness and systems thinking. A regional CC COVID-19 dashboard was developed based on publicly available data and weekly data submitted by participating facilities. Those experiencing outbreaks or supply shortages were quickly identified. As the pandemic progressed, the role of the SC shifted to address new and forecasted needs.
Results
Over 60 facilities participated in data sharing. The SC shared new guidelines, regulations, educational material, and best practices with the participating facilities. Information about testing sites, supplies, vaccination rollout, and facilities that had the capacity to accept COVID-19 patients was regularly disseminated. The SC was able to direct resources to those facilities experiencing outbreaks or supply shortages.
Conclusions
A novel learning health system of regional CC facilities enabled preparedness, situational awareness, collaboration, and rapid dissemination of best practices across pandemic phases. Such collaborative efforts can play an important role in addressing other public and preventive health challenges.
COVID-19 大流行对集中护理(CC)设施的影响尤为严重,因为这些设施都是集体生活,存在易感人群,预防资源不足,应对大流行快速发展阶段的能力有限。我们与公共卫生和医疗保健部门协调,在 14 个县的大都会地区建立了一个由 CC 设施组成的学习型卫生系统,以应对 COVID-19 带来的挑战。我们成立了一个 CC 指导委员会 (SC),该委员会代表了不同的机构和观点,包括专业护理机构、过渡性护理机构、住宅机构、监狱和避难所。指导委员会定期召开会议,并以态势感知和系统思维为指导。根据公开数据和参与机构每周提交的数据,开发了地区 CC COVID-19 面板。出现疫情或供应短缺的设施被迅速识别出来。随着大流行病的发展,自然科学部门的角色发生了转变,以满足新的和预测的需求。SC 与参与机构分享了新的指导方针、法规、教育材料和最佳实践。有关检测点、供应品、疫苗接种推广以及有能力接收 COVID-19 患者的机构的信息定期发布。由地区 CC 设施组成的新型学习型卫生系统能够在大流行病的各个阶段做好准备、了解情况、开展合作并快速传播最佳实践。这种协作努力可在应对其他公共和预防性健康挑战方面发挥重要作用。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
