Ourania Preventza MD , Jaymie Henry MD , Lubna Khan MD , Lorraine D. Cornwell MD , Katherine H. Simpson MS , Subhasis Chatterjee MD , Hiruni S. Amarasekara MS , Marc R. Moon MD , Joseph S. Coselli MD
{"title":"Unplanned readmissions, community socioeconomic factors, and their effects on long-term survival after complex thoracic aortic surgery","authors":"Ourania Preventza MD , Jaymie Henry MD , Lubna Khan MD , Lorraine D. Cornwell MD , Katherine H. Simpson MS , Subhasis Chatterjee MD , Hiruni S. Amarasekara MS , Marc R. Moon MD , Joseph S. Coselli MD","doi":"10.1016/j.jtcvs.2024.01.035","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><div>We evaluated community socioeconomic factors in patients who had unplanned readmission after undergoing proximal aortic surgery<span> (ascending aorta, aortic root, or arch).</span></div></div><div><h3>Methods</h3><div>Unplanned readmissions for any reason within 60 days of the index procedure were reviewed by race, acuity at presentation, and gender. We also evaluated 3 community socioeconomic factors: poverty, household income, and education. Kaplan-Meier survival curves were used to assess long-term survival differences by group (race, acuity, and gender).</div></div><div><h3>Results</h3><div>Among 2339 patients who underwent proximal aortic surgery during the 20-year study period and were discharged alive, our team identified 146 (6.2%) unplanned readmissions. Compared with White patients, Black patients lived in areas characterized by more widespread poverty (20.8% vs 11.1%; <em>P</em> = .0003), lower income ($42,776 vs $65,193; <em>P</em> = .0007), and fewer residents with a high school diploma (73.7% vs 90.1%; <em>P</em> < .0001). Compared with patients whose index operation was elective, patients who had urgent or emergency index procedures lived in areas with lower income ($54,425 vs $64,846; <em>P</em> = .01) and fewer residents with a high school diploma (81.1% vs 89.2%; <em>P</em> = .005). Community socioeconomic factors did not differ by gender. Four- and 6-year survival estimates were 63.1% and 63.1% for Black patients versus 89.1% and 83.0% for White patients (<em>P</em> = .0009). No significant differences by acuity or gender were found.</div></div><div><h3>Conclusions</h3><div>Among readmitted patients, Black patients and patients who had emergency surgery had less favorable community socioeconomic factors and poorer long-term survival. Earlier and more frequent follow-up in these patients should be considered. Developing off-campus clinics and specific postdischarge measures targeting these patients is important.</div></div>","PeriodicalId":49975,"journal":{"name":"Journal of Thoracic and Cardiovascular Surgery","volume":"169 1","pages":"Pages 26-35.e2"},"PeriodicalIF":4.4000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S002252232400093X","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/1 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
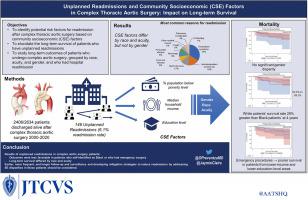
We evaluated community socioeconomic factors in patients who had unplanned readmission after undergoing proximal aortic surgery (ascending aorta, aortic root, or arch).
Methods
Unplanned readmissions for any reason within 60 days of the index procedure were reviewed by race, acuity at presentation, and gender. We also evaluated 3 community socioeconomic factors: poverty, household income, and education. Kaplan-Meier survival curves were used to assess long-term survival differences by group (race, acuity, and gender).
Results
Among 2339 patients who underwent proximal aortic surgery during the 20-year study period and were discharged alive, our team identified 146 (6.2%) unplanned readmissions. Compared with White patients, Black patients lived in areas characterized by more widespread poverty (20.8% vs 11.1%; P = .0003), lower income ($42,776 vs $65,193; P = .0007), and fewer residents with a high school diploma (73.7% vs 90.1%; P < .0001). Compared with patients whose index operation was elective, patients who had urgent or emergency index procedures lived in areas with lower income ($54,425 vs $64,846; P = .01) and fewer residents with a high school diploma (81.1% vs 89.2%; P = .005). Community socioeconomic factors did not differ by gender. Four- and 6-year survival estimates were 63.1% and 63.1% for Black patients versus 89.1% and 83.0% for White patients (P = .0009). No significant differences by acuity or gender were found.
Conclusions
Among readmitted patients, Black patients and patients who had emergency surgery had less favorable community socioeconomic factors and poorer long-term survival. Earlier and more frequent follow-up in these patients should be considered. Developing off-campus clinics and specific postdischarge measures targeting these patients is important.
期刊介绍:
The Journal of Thoracic and Cardiovascular Surgery presents original, peer-reviewed articles on diseases of the heart, great vessels, lungs and thorax with emphasis on surgical interventions. An official publication of The American Association for Thoracic Surgery and The Western Thoracic Surgical Association, the Journal focuses on techniques and developments in acquired cardiac surgery, congenital cardiac repair, thoracic procedures, heart and lung transplantation, mechanical circulatory support and other procedures.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
