Lorenzo Vittorio Rindi, Drieda Zaçe, Neva Braccialarghe, Barbara Massa, Virginia Barchi, Roberta Iannazzo, Ilenia Fato, Francesco De Maria, Dimitra Kontogiannis, Vincenzo Malagnino, Loredana Sarmati, Marco Iannetta
{"title":"Drug-Induced Progressive Multifocal Leukoencephalopathy (PML): A Systematic Review and Meta-Analysis.","authors":"Lorenzo Vittorio Rindi, Drieda Zaçe, Neva Braccialarghe, Barbara Massa, Virginia Barchi, Roberta Iannazzo, Ilenia Fato, Francesco De Maria, Dimitra Kontogiannis, Vincenzo Malagnino, Loredana Sarmati, Marco Iannetta","doi":"10.1007/s40264-023-01383-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Progressive multifocal leukoencephalopathy (PML) was first described among patients affected by hematological or solid tumors. Following the human immunodeficiency virus (HIV) epidemic, people living with HIV have represented most cases for more than a decade. With the diffusion of highly active antiretroviral therapy, this group progressively decreased in favor of patients undergoing treatment with targeted therapy/immunomodulators. In this systematic review and meta-analysis, the objective was to assess which drugs are most frequently related to PML development, and report the incidence of drug-induced PML through a meta-analytic approach.</p><p><strong>Methods: </strong>The electronic databases MEDLINE, EMBASE, ClinicalTrials.gov, Web of Science and the Canadian Agency for Drugs and Technologies in Health Database (CADTH) were searched up to May 10, 2022. Articles that reported the risk of PML development after treatment with immunomodulatory drugs, including patients of both sexes under the age of 80 years, affected by any pathology except HIV, primary immunodeficiencies or malignancies, were included in the review. The incidence of drug-induced PML was calculated based on PML cases and total number of patients observed per 100 persons and the observation time. Random-effect metanalyses were conducted for each drug reporting pooled incidence with 95% confidence intervals (CI) and median (interquartile range [IQR]) of the observation time. Heterogeneity was measured by I<sup>2</sup> statistics. Publication bias was examined through funnel plots and Egger's test.</p><p><strong>Results: </strong>A total of 103 studies were included in the systematic review. In our analysis, we found no includible study reporting cases of PML during the course of treatment with ocrelizumab, vedolizumab, abrilumab, ontamalimab, teriflunomide, daclizumab, inebilizumab, basiliximab, tacrolimus, belimumab, infliximab, firategrast, disulone, azathioprine or danazole. Dalfampridine, glatiramer acetate, dimethyl fumarate and fingolimod show a relatively safe profile, although some cases of PML have been reported. The meta-analysis showed an incidence of PML cases among patients undergoing rituximab treatment for multiple sclerosis (MS) of 0.01 cases/100 persons (95% CI - 0.08 to 0.09; I<sup>2</sup> = 20.4%; p = 0.25) for a median observation period of 23.5 months (IQR 22.1-42.1). Treatment of MS with natalizumab carried a PML risk of 0.33 cases/100 persons (95% CI 0.29-0.37; I<sup>2</sup> = 50%; p = 0.003) for a median observation period of 44.1 months (IQR 28.4-60) and a mean number of doses of 36.3 (standard deviation [SD] ± 20.7). When comparing data about patients treated with standard interval dosing (SID) and extended interval dosing (EID), the latter appears to carry a smaller risk of PML, that is, 0.08 cases/100 persons (95% CI 0.0-0.15) for EID versus 0.3 cases/100 persons (95% CI 0.25-0.34) for SID.</p><p><strong>Conclusions: </strong>A higher risk of drug-related PML in patients whose immune system is not additionally depressed by means of neoplasms, HIV or concomitant medications is found in the neurological field. This risk is higher in MS treatment, and specifically during long-term natalizumab therapy. While this drug is still routinely prescribed in this field, considering the efficacy in reducing MS relapses, in other areas it could play a smaller role, and be gradually replaced by other safer and more recently approved agents.</p>","PeriodicalId":11382,"journal":{"name":"Drug Safety","volume":" ","pages":"333-354"},"PeriodicalIF":3.8000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40264-023-01383-4","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/7 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Progressive multifocal leukoencephalopathy (PML) was first described among patients affected by hematological or solid tumors. Following the human immunodeficiency virus (HIV) epidemic, people living with HIV have represented most cases for more than a decade. With the diffusion of highly active antiretroviral therapy, this group progressively decreased in favor of patients undergoing treatment with targeted therapy/immunomodulators. In this systematic review and meta-analysis, the objective was to assess which drugs are most frequently related to PML development, and report the incidence of drug-induced PML through a meta-analytic approach.
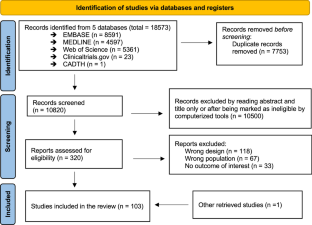
Methods: The electronic databases MEDLINE, EMBASE, ClinicalTrials.gov, Web of Science and the Canadian Agency for Drugs and Technologies in Health Database (CADTH) were searched up to May 10, 2022. Articles that reported the risk of PML development after treatment with immunomodulatory drugs, including patients of both sexes under the age of 80 years, affected by any pathology except HIV, primary immunodeficiencies or malignancies, were included in the review. The incidence of drug-induced PML was calculated based on PML cases and total number of patients observed per 100 persons and the observation time. Random-effect metanalyses were conducted for each drug reporting pooled incidence with 95% confidence intervals (CI) and median (interquartile range [IQR]) of the observation time. Heterogeneity was measured by I2 statistics. Publication bias was examined through funnel plots and Egger's test.
Results: A total of 103 studies were included in the systematic review. In our analysis, we found no includible study reporting cases of PML during the course of treatment with ocrelizumab, vedolizumab, abrilumab, ontamalimab, teriflunomide, daclizumab, inebilizumab, basiliximab, tacrolimus, belimumab, infliximab, firategrast, disulone, azathioprine or danazole. Dalfampridine, glatiramer acetate, dimethyl fumarate and fingolimod show a relatively safe profile, although some cases of PML have been reported. The meta-analysis showed an incidence of PML cases among patients undergoing rituximab treatment for multiple sclerosis (MS) of 0.01 cases/100 persons (95% CI - 0.08 to 0.09; I2 = 20.4%; p = 0.25) for a median observation period of 23.5 months (IQR 22.1-42.1). Treatment of MS with natalizumab carried a PML risk of 0.33 cases/100 persons (95% CI 0.29-0.37; I2 = 50%; p = 0.003) for a median observation period of 44.1 months (IQR 28.4-60) and a mean number of doses of 36.3 (standard deviation [SD] ± 20.7). When comparing data about patients treated with standard interval dosing (SID) and extended interval dosing (EID), the latter appears to carry a smaller risk of PML, that is, 0.08 cases/100 persons (95% CI 0.0-0.15) for EID versus 0.3 cases/100 persons (95% CI 0.25-0.34) for SID.
Conclusions: A higher risk of drug-related PML in patients whose immune system is not additionally depressed by means of neoplasms, HIV or concomitant medications is found in the neurological field. This risk is higher in MS treatment, and specifically during long-term natalizumab therapy. While this drug is still routinely prescribed in this field, considering the efficacy in reducing MS relapses, in other areas it could play a smaller role, and be gradually replaced by other safer and more recently approved agents.
期刊介绍:
Drug Safety is the official journal of the International Society of Pharmacovigilance. The journal includes:
Overviews of contentious or emerging issues.
Comprehensive narrative reviews that provide an authoritative source of information on epidemiology, clinical features, prevention and management of adverse effects of individual drugs and drug classes.
In-depth benefit-risk assessment of adverse effect and efficacy data for a drug in a defined therapeutic area.
Systematic reviews (with or without meta-analyses) that collate empirical evidence to answer a specific research question, using explicit, systematic methods as outlined by the PRISMA statement.
Original research articles reporting the results of well-designed studies in disciplines such as pharmacoepidemiology, pharmacovigilance, pharmacology and toxicology, and pharmacogenomics.
Editorials and commentaries on topical issues.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in Drug Safety Drugs may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
