Kathryn McGillen , Nabeal Aljabban , Robert Wu , Benjamin Shin , Ian Schreibman , Franklin Luke , James Birkholz
{"title":"Addition of contrast in ultrasound screening for hepatocellular carcinoma","authors":"Kathryn McGillen , Nabeal Aljabban , Robert Wu , Benjamin Shin , Ian Schreibman , Franklin Luke , James Birkholz","doi":"10.1016/j.redii.2023.100039","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>Screening ultrasound for hepatocellular carcinoma (HCC) identifies lesions which require further characterization by a contrast-enhanced exam to non-invasively diagnose HCC. While ultrasound is recommended in screening, some HCC can be occult on grayscale imaging. The purpose of this study was to determine if the addition of ultrasound contrast (sulfahexafluoride) to screening ultrasound for HCC can identify more HCC lesions than grayscale sonographic imaging alone.</p></div><div><h3>Methods</h3><p>All HCC screening ultrasounds that also had contrast were evaluated in this retrospective study. Patients with a focal lesion seen only after administration of contrast (OAC) were noted, as well as any follow-up imaging or pathology results. Additional variables collected included patient demographics, cirrhosis type, and laboratory values.</p></div><div><h3>Results</h3><p>230 unique patients were included, of which 160 had imaging or pathology follow-up. 18 of these patients had an OAC lesion, of which 17 had follow-up. Among these OACs, there was one LIRADS M lesion (1/18, 5.6 %) and one bland portal vein thrombus identified, which were both confirmed on follow-up imaging. All LIRADS 4 OAC lesions were downgraded. No additional HCC were identified on follow-up imaging or pathology of these patients.</p></div><div><h3>Conclusion</h3><p>Addition of contrast to screening ultrasound did identify additional lesions, portal vein thrombus, and high grade malignancy. However, as the incidence of OAC lesions was low (7.8 %, 18/230) and most of the lesions were not malignant, addition of post contrast sweeps through the liver is of low value in the low to medium at-risk cirrhotic population in identifying occult HCC.</p></div>","PeriodicalId":74676,"journal":{"name":"Research in diagnostic and interventional imaging","volume":"9 ","pages":"Article 100039"},"PeriodicalIF":0.0000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2772652523000182/pdfft?md5=45ff1f5c2f11de69586c2f7ff8c67cb7&pid=1-s2.0-S2772652523000182-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Research in diagnostic and interventional imaging","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2772652523000182","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/7 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
Screening ultrasound for hepatocellular carcinoma (HCC) identifies lesions which require further characterization by a contrast-enhanced exam to non-invasively diagnose HCC. While ultrasound is recommended in screening, some HCC can be occult on grayscale imaging. The purpose of this study was to determine if the addition of ultrasound contrast (sulfahexafluoride) to screening ultrasound for HCC can identify more HCC lesions than grayscale sonographic imaging alone.
Methods
All HCC screening ultrasounds that also had contrast were evaluated in this retrospective study. Patients with a focal lesion seen only after administration of contrast (OAC) were noted, as well as any follow-up imaging or pathology results. Additional variables collected included patient demographics, cirrhosis type, and laboratory values.
Results
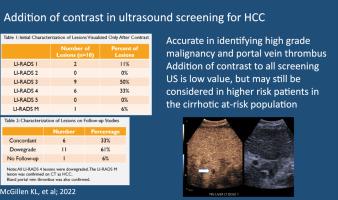
230 unique patients were included, of which 160 had imaging or pathology follow-up. 18 of these patients had an OAC lesion, of which 17 had follow-up. Among these OACs, there was one LIRADS M lesion (1/18, 5.6 %) and one bland portal vein thrombus identified, which were both confirmed on follow-up imaging. All LIRADS 4 OAC lesions were downgraded. No additional HCC were identified on follow-up imaging or pathology of these patients.
Conclusion
Addition of contrast to screening ultrasound did identify additional lesions, portal vein thrombus, and high grade malignancy. However, as the incidence of OAC lesions was low (7.8 %, 18/230) and most of the lesions were not malignant, addition of post contrast sweeps through the liver is of low value in the low to medium at-risk cirrhotic population in identifying occult HCC.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
