Christopher L Boswell, Sarah A Minteer, Svetlana Herasevich, Juan P Garcia-Mendez, Yue Dong, Ognjen Gajic, Amelia K Barwise
{"title":"Early Prevention of Critical Illness in Older Adults: Adaptation and Pilot Testing of an Electronic Risk Score and Checklist.","authors":"Christopher L Boswell, Sarah A Minteer, Svetlana Herasevich, Juan P Garcia-Mendez, Yue Dong, Ognjen Gajic, Amelia K Barwise","doi":"10.1177/21501319241231238","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Given limited critical care resources and an aging population, early interventions to prevent critical illness are vital. In this work, we measured post-implementation outcomes after introducing a novel electronic scoring system (Elders Risk Assessment-ERA) and a risk-factor checklist, Checklist for Early Recognition and Treatment of Acute Illness (CERTAIN), to detect older patients at high risk of critical illness in a primary care setting.</p><p><strong>Methods: </strong>The study was conducted at a family medicine clinic in Kasson, MN. The ADAPT-ITT framework was used to modify the CERTAIN checklist for primary care during 2 co-design workshops involving interdisciplinary clinicians, held in April 2023. The ERA score and modified CERTAIN checklist were implemented between May and July 2023 and identify and assess all patients age ≥60 years at risk of critical illness during their primary care visits. Implementation outcomes were evaluated at the end of the study via an anonymous survey and EHR data extraction.</p><p><strong>Results: </strong>Fourteen clinicians participated in 2 co-design workshops. A total of 19 clinicians participated in a post-pilot survey. All survey items were rated on a 5-point Likert type scale. Mean acceptability of the ERA score and checklist was rated 3.35 (SD = 0.75) and 3.09 (SD = 0.64), respectively. Appropriateness had a mean rating of 3.38 (SD = 0.82) for the ERA score and 3.19 (SD = 0.59) for the checklist. Mean feasibility was rated 3.38(SD = 0.85) and 2.92 (SD = 0.76) for the ERA score and checklist, respectively. The adoption rate was 50% (19/38) among clinicians, but the reach was low at 17% (49/289) of eligible patients.</p><p><strong>Conclusions: </strong>This pilot study evaluated the implementation of an intervention that introduced the ERA score and CERTAIN checklist into a primary care practice. Results indicate moderate acceptability, appropriateness, and feasibility of the ERA score, and similar ratings for the checklist, with slightly lower feasibility. While checklist adoption was moderate, reach was limited, indicating inconsistent use.</p><p><strong>Recommendations: </strong>We plan to use the open-ended resurvey responses to further modify the CERTAIN-FM checklist and implementation process. The ADAPT-ITT framework is a useful model for adapting the checklist to meet the primary care clinician needs.</p>","PeriodicalId":46723,"journal":{"name":"Journal of Primary Care and Community Health","volume":"15 ","pages":"21501319241231238"},"PeriodicalIF":2.5000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10863481/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Primary Care and Community Health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/21501319241231238","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Given limited critical care resources and an aging population, early interventions to prevent critical illness are vital. In this work, we measured post-implementation outcomes after introducing a novel electronic scoring system (Elders Risk Assessment-ERA) and a risk-factor checklist, Checklist for Early Recognition and Treatment of Acute Illness (CERTAIN), to detect older patients at high risk of critical illness in a primary care setting.
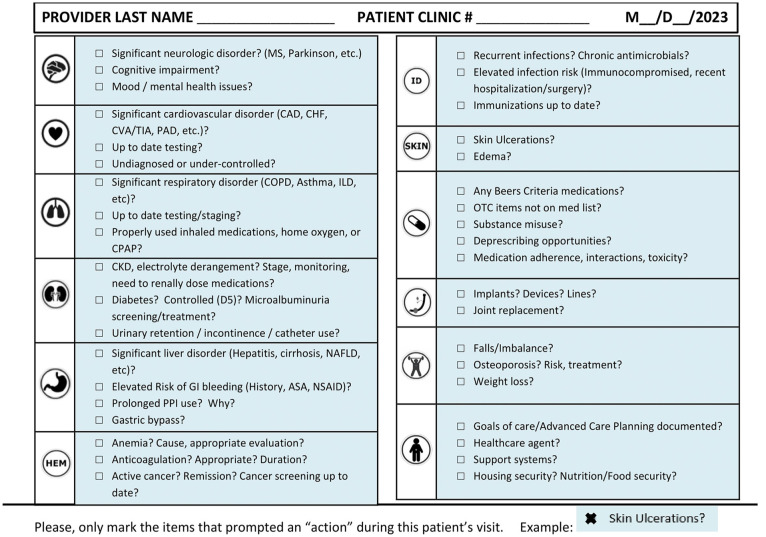
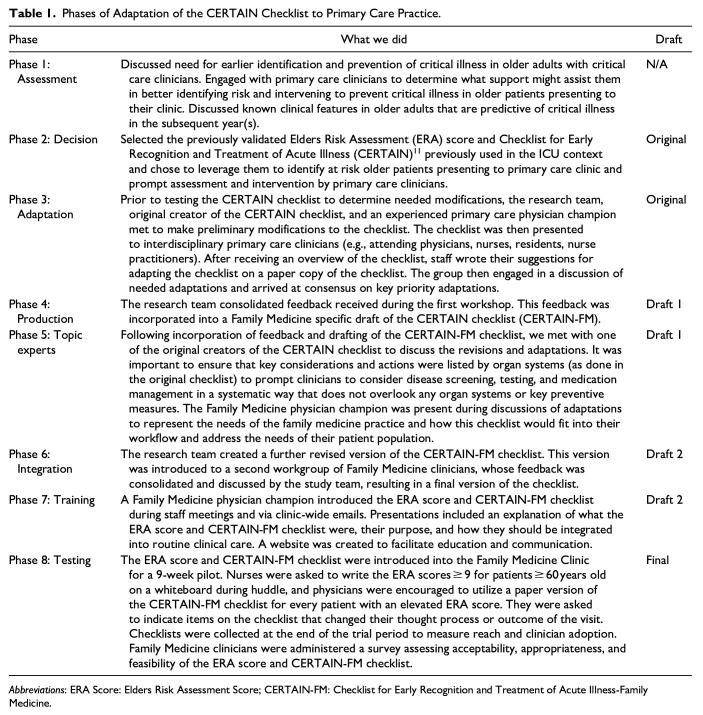
Methods: The study was conducted at a family medicine clinic in Kasson, MN. The ADAPT-ITT framework was used to modify the CERTAIN checklist for primary care during 2 co-design workshops involving interdisciplinary clinicians, held in April 2023. The ERA score and modified CERTAIN checklist were implemented between May and July 2023 and identify and assess all patients age ≥60 years at risk of critical illness during their primary care visits. Implementation outcomes were evaluated at the end of the study via an anonymous survey and EHR data extraction.
Results: Fourteen clinicians participated in 2 co-design workshops. A total of 19 clinicians participated in a post-pilot survey. All survey items were rated on a 5-point Likert type scale. Mean acceptability of the ERA score and checklist was rated 3.35 (SD = 0.75) and 3.09 (SD = 0.64), respectively. Appropriateness had a mean rating of 3.38 (SD = 0.82) for the ERA score and 3.19 (SD = 0.59) for the checklist. Mean feasibility was rated 3.38(SD = 0.85) and 2.92 (SD = 0.76) for the ERA score and checklist, respectively. The adoption rate was 50% (19/38) among clinicians, but the reach was low at 17% (49/289) of eligible patients.
Conclusions: This pilot study evaluated the implementation of an intervention that introduced the ERA score and CERTAIN checklist into a primary care practice. Results indicate moderate acceptability, appropriateness, and feasibility of the ERA score, and similar ratings for the checklist, with slightly lower feasibility. While checklist adoption was moderate, reach was limited, indicating inconsistent use.
Recommendations: We plan to use the open-ended resurvey responses to further modify the CERTAIN-FM checklist and implementation process. The ADAPT-ITT framework is a useful model for adapting the checklist to meet the primary care clinician needs.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
