Comparing the performance of a deep learning-based lung gross tumour volume segmentation algorithm before and after transfer learning in a new hospital.
Chaitanya Kulkarni, Umesh Sherkhane, Vinay Jaiswar, Sneha Mithun, Dinesh Mysore Siddu, Venkatesh Rangarajan, Andre Dekker, Alberto Traverso, Ashish Jha, Leonard Wee
{"title":"Comparing the performance of a deep learning-based lung gross tumour volume segmentation algorithm before and after transfer learning in a new hospital.","authors":"Chaitanya Kulkarni, Umesh Sherkhane, Vinay Jaiswar, Sneha Mithun, Dinesh Mysore Siddu, Venkatesh Rangarajan, Andre Dekker, Alberto Traverso, Ashish Jha, Leonard Wee","doi":"10.1093/bjro/tzad008","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Radiation therapy for lung cancer requires a gross tumour volume (GTV) to be carefully outlined by a skilled radiation oncologist (RO) to accurately pinpoint high radiation dose to a malignant mass while simultaneously minimizing radiation damage to adjacent normal tissues. This is manually intensive and tedious however, it is feasible to train a deep learning (DL) neural network that could assist ROs to delineate the GTV. However, DL trained on large openly accessible data sets might not perform well when applied to a superficially similar task but in a different clinical setting. In this work, we tested the performance of DL automatic lung GTV segmentation model trained on open-access Dutch data when used on Indian patients from a large public tertiary hospital, and hypothesized that <i>generic</i> DL performance could be improved for a specific <i>local</i> clinical context, by means of modest transfer-learning on a small representative local subset.</p><p><strong>Methods: </strong>X-ray computed tomography (CT) series in a public data set called \"NSCLC-Radiomics\" from The Cancer Imaging Archive was first used to train a DL-based lung GTV segmentation model (Model 1). Its performance was assessed using a different open access data set (Interobserver1) of Dutch subjects plus a private Indian data set from a local tertiary hospital (Test Set 2). Another Indian data set (Retrain Set 1) was used to fine-tune the former DL model using a transfer learning method. The Indian data sets were taken from CT of a hybrid scanner based in nuclear medicine, but the GTV was drawn by skilled Indian ROs. The final (after fine-tuning) model (Model 2) was then re-evaluated in \"Interobserver1\" and \"Test Set 2.\" Dice similarity coefficient (DSC), precision, and recall were used as geometric segmentation performance metrics.</p><p><strong>Results: </strong>Model 1 trained exclusively on Dutch scans showed a significant fall in performance when tested on \"Test Set 2.\" However, the DSC of Model 2 recovered by 14 percentage points when evaluated in the same test set. Precision and recall showed a similar rebound of performance after transfer learning, in spite of using a comparatively small sample size. The performance of both models, before and after the fine-tuning, did not significantly change the segmentation performance in \"Interobserver1.\"</p><p><strong>Conclusions: </strong>A large public open-access data set was used to train a generic DL model for lung GTV segmentation, but this did not perform well initially in the Indian clinical context. Using transfer learning methods, it was feasible to efficiently and easily fine-tune the generic model using only a small number of local examples from the Indian hospital. This led to a recovery of some of the geometric segmentation performance, but the tuning did not appear to affect the performance of the model in another open-access data set.</p><p><strong>Advances in knowledge: </strong>Caution is needed when using models trained on large volumes of international data in a local clinical setting, even when that training data set is of good quality. Minor differences in scan acquisition and clinician delineation preferences may result in an apparent drop in performance. However, DL models have the advantage of being efficiently \"adapted\" from a generic to a locally specific context, with only a small amount of fine-tuning by means of transfer learning on a small local institutional data set.</p>","PeriodicalId":72419,"journal":{"name":"BJR open","volume":"6 1","pages":"tzad008"},"PeriodicalIF":2.1000,"publicationDate":"2023-12-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10860512/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJR open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/bjro/tzad008","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
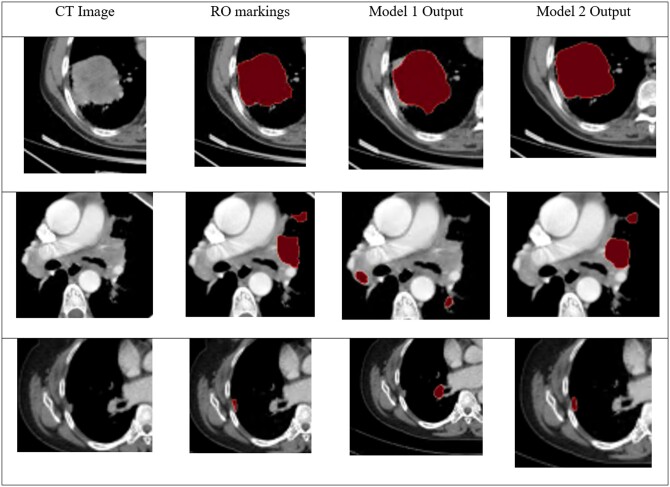
Objectives: Radiation therapy for lung cancer requires a gross tumour volume (GTV) to be carefully outlined by a skilled radiation oncologist (RO) to accurately pinpoint high radiation dose to a malignant mass while simultaneously minimizing radiation damage to adjacent normal tissues. This is manually intensive and tedious however, it is feasible to train a deep learning (DL) neural network that could assist ROs to delineate the GTV. However, DL trained on large openly accessible data sets might not perform well when applied to a superficially similar task but in a different clinical setting. In this work, we tested the performance of DL automatic lung GTV segmentation model trained on open-access Dutch data when used on Indian patients from a large public tertiary hospital, and hypothesized that generic DL performance could be improved for a specific local clinical context, by means of modest transfer-learning on a small representative local subset.
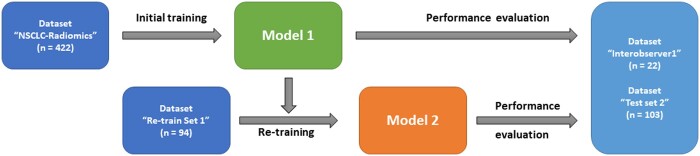
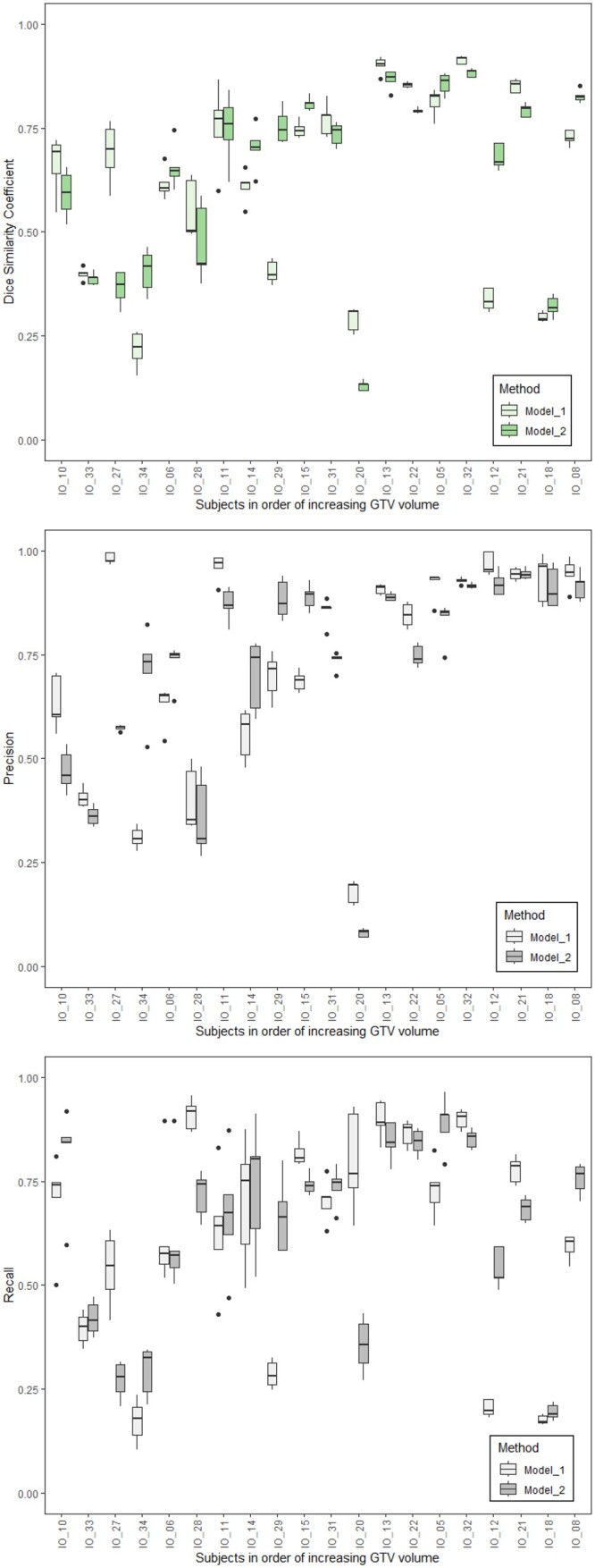
Methods: X-ray computed tomography (CT) series in a public data set called "NSCLC-Radiomics" from The Cancer Imaging Archive was first used to train a DL-based lung GTV segmentation model (Model 1). Its performance was assessed using a different open access data set (Interobserver1) of Dutch subjects plus a private Indian data set from a local tertiary hospital (Test Set 2). Another Indian data set (Retrain Set 1) was used to fine-tune the former DL model using a transfer learning method. The Indian data sets were taken from CT of a hybrid scanner based in nuclear medicine, but the GTV was drawn by skilled Indian ROs. The final (after fine-tuning) model (Model 2) was then re-evaluated in "Interobserver1" and "Test Set 2." Dice similarity coefficient (DSC), precision, and recall were used as geometric segmentation performance metrics.
Results: Model 1 trained exclusively on Dutch scans showed a significant fall in performance when tested on "Test Set 2." However, the DSC of Model 2 recovered by 14 percentage points when evaluated in the same test set. Precision and recall showed a similar rebound of performance after transfer learning, in spite of using a comparatively small sample size. The performance of both models, before and after the fine-tuning, did not significantly change the segmentation performance in "Interobserver1."
Conclusions: A large public open-access data set was used to train a generic DL model for lung GTV segmentation, but this did not perform well initially in the Indian clinical context. Using transfer learning methods, it was feasible to efficiently and easily fine-tune the generic model using only a small number of local examples from the Indian hospital. This led to a recovery of some of the geometric segmentation performance, but the tuning did not appear to affect the performance of the model in another open-access data set.
Advances in knowledge: Caution is needed when using models trained on large volumes of international data in a local clinical setting, even when that training data set is of good quality. Minor differences in scan acquisition and clinician delineation preferences may result in an apparent drop in performance. However, DL models have the advantage of being efficiently "adapted" from a generic to a locally specific context, with only a small amount of fine-tuning by means of transfer learning on a small local institutional data set.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
