Antoine Leveque, Delphine Rolland, Marie-Pierre Ledoux, Célestine Simand, Alice Eischen, Caroline Mayeur-Rousse
{"title":"Transient red blood cell agglutination after Magrolimab administration in acute myeloid leukemia","authors":"Antoine Leveque, Delphine Rolland, Marie-Pierre Ledoux, Célestine Simand, Alice Eischen, Caroline Mayeur-Rousse","doi":"10.1111/ijlh.14252","DOIUrl":null,"url":null,"abstract":"<p>A 65-year-old female patient with Burkitt lymphoma history in 2020 (currently in remission) was diagnosed with post-cytotoxic therapy acute myeloid leukemia (AML) in June 2023. The patient agreed to be included in ENHANCE-3, a double-blind randomized protocol designed to evaluate magrolimab safety and efficacy in combination with venetoclax and azacitidine in previously untreated AML patients ineligible for intensive therapy. Placebo or magrolimab were administrated in step-up doses for 2 weeks in association with usual doses of venetoclax and azacitidine, then gradual spaced. Magrolimab, a monoclonal anti-CD47 antibody, blocks the « don't eat me » signal from tumor cells to signal-regulatory protein alpha (SIRPα) positive immune cells.</p><p>For her hematological follow-up, complete blood count (CBC) were run on XN-9000 SYSMEX analyzer. A CBC interference was observed with red blood cell (RBC) agglutination from 2 to 10 h (H + 2 to H + 10) after the first placebo/magrolimab administration. Two RBC populations were identified on both optic and impedance channels: the usual RBC population, and an agglutinated one (Figure 1A,B). None of pre-analytic performed treatments (plasma substitution with saline solution, 37°C heating, citrate-based anticoagulation) corrected this interference. Therefore, none of the RBC parameters (except for hemoglobin level at 75 g/L) could be determined at H + 2 timepoint. Macroscopic and microscopic blood smear examinations confirmed RBC agglutination (Figure 1C–E). There was no biological evidence of hemolysis (haptoglobin, LDH, and bilirubin within normal ranges). Qualitative interferences resolved almost fully at H + 10 (Figure 1F–J). At that time, the hemoglobin level was 91 g/L and RBC parameters were acceptable only within the optic channel with RBC-optic at 2.77 Tera/L (T/L). Mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC) and mean corpuscular volume (MCV) were recalculated at 32.9 pg, 368 g/L and 89.4 fL, respectively. The same interference reoccurred after each magrolimab or placebo administration to a lesser extent and completely regressed within 24 h. However, a probable untrue decrease in hemoglobin level (−24 g/L) was only detected after the first administration.</p><p>Since CD47 is highly expressed by RBC, magrolimab early clinical trials have already highlighted RBC agglutinations during ABO blood typing.<span><sup>1, 2</sup></span> Although this phenomena has never been reported for RBC parameters yet, we deduced the patient received magrolimab. Physicians should be aware of such interference, particularly in context of transfusion decision for AML patients, and repeat if necessary the CBC.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":14120,"journal":{"name":"International Journal of Laboratory Hematology","volume":"46 4","pages":"591-592"},"PeriodicalIF":2.3000,"publicationDate":"2024-02-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ijlh.14252","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Laboratory Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ijlh.14252","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
A 65-year-old female patient with Burkitt lymphoma history in 2020 (currently in remission) was diagnosed with post-cytotoxic therapy acute myeloid leukemia (AML) in June 2023. The patient agreed to be included in ENHANCE-3, a double-blind randomized protocol designed to evaluate magrolimab safety and efficacy in combination with venetoclax and azacitidine in previously untreated AML patients ineligible for intensive therapy. Placebo or magrolimab were administrated in step-up doses for 2 weeks in association with usual doses of venetoclax and azacitidine, then gradual spaced. Magrolimab, a monoclonal anti-CD47 antibody, blocks the « don't eat me » signal from tumor cells to signal-regulatory protein alpha (SIRPα) positive immune cells.
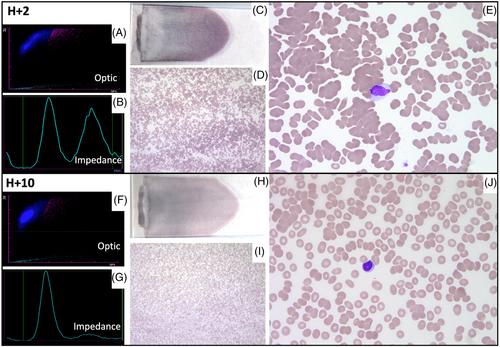
For her hematological follow-up, complete blood count (CBC) were run on XN-9000 SYSMEX analyzer. A CBC interference was observed with red blood cell (RBC) agglutination from 2 to 10 h (H + 2 to H + 10) after the first placebo/magrolimab administration. Two RBC populations were identified on both optic and impedance channels: the usual RBC population, and an agglutinated one (Figure 1A,B). None of pre-analytic performed treatments (plasma substitution with saline solution, 37°C heating, citrate-based anticoagulation) corrected this interference. Therefore, none of the RBC parameters (except for hemoglobin level at 75 g/L) could be determined at H + 2 timepoint. Macroscopic and microscopic blood smear examinations confirmed RBC agglutination (Figure 1C–E). There was no biological evidence of hemolysis (haptoglobin, LDH, and bilirubin within normal ranges). Qualitative interferences resolved almost fully at H + 10 (Figure 1F–J). At that time, the hemoglobin level was 91 g/L and RBC parameters were acceptable only within the optic channel with RBC-optic at 2.77 Tera/L (T/L). Mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC) and mean corpuscular volume (MCV) were recalculated at 32.9 pg, 368 g/L and 89.4 fL, respectively. The same interference reoccurred after each magrolimab or placebo administration to a lesser extent and completely regressed within 24 h. However, a probable untrue decrease in hemoglobin level (−24 g/L) was only detected after the first administration.
Since CD47 is highly expressed by RBC, magrolimab early clinical trials have already highlighted RBC agglutinations during ABO blood typing.1, 2 Although this phenomena has never been reported for RBC parameters yet, we deduced the patient received magrolimab. Physicians should be aware of such interference, particularly in context of transfusion decision for AML patients, and repeat if necessary the CBC.
期刊介绍:
The International Journal of Laboratory Hematology provides a forum for the communication of new developments, research topics and the practice of laboratory haematology.
The journal publishes invited reviews, full length original articles, and correspondence.
The International Journal of Laboratory Hematology is the official journal of the International Society for Laboratory Hematology, which addresses the following sub-disciplines: cellular analysis, flow cytometry, haemostasis and thrombosis, molecular diagnostics, haematology informatics, haemoglobinopathies, point of care testing, standards and guidelines.
The journal was launched in 2006 as the successor to Clinical and Laboratory Hematology, which was first published in 1979. An active and positive editorial policy ensures that work of a high scientific standard is reported, in order to bridge the gap between practical and academic aspects of laboratory haematology.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
