Daniele Sartori, Jeffrey K Aronson, Nils Erlanson, G Niklas Norén, Igho J Onakpoya
{"title":"A Comparison of Signals of Designated Medical Events and Non-designated Medical Events: Results from a Scoping Review.","authors":"Daniele Sartori, Jeffrey K Aronson, Nils Erlanson, G Niklas Norén, Igho J Onakpoya","doi":"10.1007/s40264-024-01403-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction and objective: </strong>The European Medicines Agency (EMA) maintains a list of designated medical events (DMEs), events that are inherently serious and are prioritized for signal detection, irrespective of statistical criteria. We have analysed the results of our previously published scoping review to determine whether DME signals differ from those of other adverse events in terms of time to communication and characteristics of supporting reports of suspected adverse drug reactions.</p><p><strong>Methods: </strong>For all signals, we obtained the launch year of medicinal products from textbooks or regulatory agencies, extracted the year of the first report in VigiBase and calculated the interval between the first report and communication (time to communication, TTC). We further retrieved the average completeness (via vigiGrade) of the reports in each case series in the years before the communication. We categorised as DME signals those concerning an event in the EMA's list. We described the two groups of signals using medians and interquartile ranges (IQR) and compared them using the Brunner-Munzel test, calculating 95% confidence intervals (95% CI) and P values.</p><p><strong>Results: </strong>Of 4520 signals, 919 concerned DMEs and 3601 concerned non-DMEs. Signals of DMEs were supported by a median of 15 reports (IQR 6-38 reports) with a completeness score of 0.52 (IQR 0.43-0.62) and signals of non-DMEs by 20 reports (IQR 6-84 reports) with a completeness score of 0.46 (IQR 0.38-0.56). The probability that a random DME signal was supported by fewer reports than non-DME signals was 0.56 (95% CI 0.54-0.58, P < 0.001) and that of one having lower average completeness was 0.39 (95% CI 0.36-0.41, P < 0.001). The median TTCs of DME and non-DME signals did not differ (10 years), but the TTC was as low as 2 years when signals (irrespective of classification) were supported by reports whose average completeness was > 0.80.</p><p><strong>Conclusions: </strong>Signals of designated medical events were supported by fewer reports and higher completeness scores than signals of other adverse events. Although statistically significant, the differences in effect sizes between the two groups were small. This suggests that listing certain adverse events as DMEs is not having the expected effect of encouraging a focus on reports of the types of suspected adverse reactions that deserve special attention. Further enhancing the completeness of the reports of suspected adverse drug reactions supporting signals of designated medical events might shorten their time to communication and reduce the number of reports required to support them.</p>","PeriodicalId":11382,"journal":{"name":"Drug Safety","volume":" ","pages":"475-485"},"PeriodicalIF":3.8000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11018663/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40264-024-01403-x","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/24 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction and objective: The European Medicines Agency (EMA) maintains a list of designated medical events (DMEs), events that are inherently serious and are prioritized for signal detection, irrespective of statistical criteria. We have analysed the results of our previously published scoping review to determine whether DME signals differ from those of other adverse events in terms of time to communication and characteristics of supporting reports of suspected adverse drug reactions.
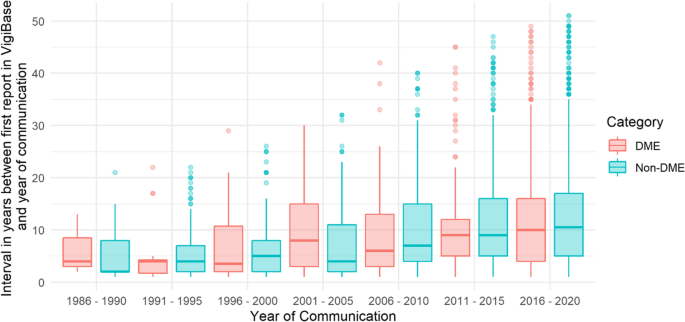
Methods: For all signals, we obtained the launch year of medicinal products from textbooks or regulatory agencies, extracted the year of the first report in VigiBase and calculated the interval between the first report and communication (time to communication, TTC). We further retrieved the average completeness (via vigiGrade) of the reports in each case series in the years before the communication. We categorised as DME signals those concerning an event in the EMA's list. We described the two groups of signals using medians and interquartile ranges (IQR) and compared them using the Brunner-Munzel test, calculating 95% confidence intervals (95% CI) and P values.
Results: Of 4520 signals, 919 concerned DMEs and 3601 concerned non-DMEs. Signals of DMEs were supported by a median of 15 reports (IQR 6-38 reports) with a completeness score of 0.52 (IQR 0.43-0.62) and signals of non-DMEs by 20 reports (IQR 6-84 reports) with a completeness score of 0.46 (IQR 0.38-0.56). The probability that a random DME signal was supported by fewer reports than non-DME signals was 0.56 (95% CI 0.54-0.58, P < 0.001) and that of one having lower average completeness was 0.39 (95% CI 0.36-0.41, P < 0.001). The median TTCs of DME and non-DME signals did not differ (10 years), but the TTC was as low as 2 years when signals (irrespective of classification) were supported by reports whose average completeness was > 0.80.
Conclusions: Signals of designated medical events were supported by fewer reports and higher completeness scores than signals of other adverse events. Although statistically significant, the differences in effect sizes between the two groups were small. This suggests that listing certain adverse events as DMEs is not having the expected effect of encouraging a focus on reports of the types of suspected adverse reactions that deserve special attention. Further enhancing the completeness of the reports of suspected adverse drug reactions supporting signals of designated medical events might shorten their time to communication and reduce the number of reports required to support them.
期刊介绍:
Drug Safety is the official journal of the International Society of Pharmacovigilance. The journal includes:
Overviews of contentious or emerging issues.
Comprehensive narrative reviews that provide an authoritative source of information on epidemiology, clinical features, prevention and management of adverse effects of individual drugs and drug classes.
In-depth benefit-risk assessment of adverse effect and efficacy data for a drug in a defined therapeutic area.
Systematic reviews (with or without meta-analyses) that collate empirical evidence to answer a specific research question, using explicit, systematic methods as outlined by the PRISMA statement.
Original research articles reporting the results of well-designed studies in disciplines such as pharmacoepidemiology, pharmacovigilance, pharmacology and toxicology, and pharmacogenomics.
Editorials and commentaries on topical issues.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in Drug Safety Drugs may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
