Comparing Anesthesia and Surgery Controlled Time for Primary Total Knee and Hip Arthroplasty Between an Academic Medical Center and a Community Hospital: Retrospective Cohort Study.
Thy B Nguyen, Nathaen Weitzel, Craig Hogan, Rachel M Kacmar, Kayla M Williamson, Jack Pattee, Vesna Jevtovic-Todorovic, Colby G Simmons, Adeel Ahmad Faruki
{"title":"Comparing Anesthesia and Surgery Controlled Time for Primary Total Knee and Hip Arthroplasty Between an Academic Medical Center and a Community Hospital: Retrospective Cohort Study.","authors":"Thy B Nguyen, Nathaen Weitzel, Craig Hogan, Rachel M Kacmar, Kayla M Williamson, Jack Pattee, Vesna Jevtovic-Todorovic, Colby G Simmons, Adeel Ahmad Faruki","doi":"10.2196/45126","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Osteoarthritis is a significant cause of disability, resulting in increased joint replacement surgeries and health care costs. Establishing benchmarks that more accurately predict surgical duration could help to decrease costs, maximize efficiency, and improve patient experience. We compared the anesthesia-controlled time (ACT) and surgery-controlled time (SCT) of primary total knee (TKA) and total hip arthroplasties (THA) between an academic medical center (AMC) and a community hospital (CH) for 2 orthopedic surgeons.</p><p><strong>Objective: </strong>This study aims to validate and compare benchmarking times for ACT and SCT in a single patient population at both an AMC and a CH.</p><p><strong>Methods: </strong>This retrospective 2-center observational cohort study was conducted at the University of Colorado Hospital (AMC) and UCHealth Broomfield Hospital (CH). Cases with current procedural terminology codes for THA and TKA between January 1, 2019, and December 31, 2020, were assessed. Cases with missing data were excluded. The primary outcomes were ACT and SCT. Primary outcomes were tested for association with covariates of interest. The primary covariate of interest was the location of the procedure (CH vs AMC); secondary covariates of interest included the American Society of Anesthesiologists (ASA) classification and anesthetic type. Linear regression models were used to assess the relationships.</p><p><strong>Results: </strong>Two surgeons performed 1256 cases at the AMC and CH. A total of 10 THA cases and 12 TKA cases were excluded due to missing data. After controlling for surgeon, the ACT was greater at the AMC for THA by 3.77 minutes and for TKA by 3.58 minutes (P<.001). SCT was greater at the AMC for THA by 11.14 minutes and for TKA by 14.04 minutes (P<.001). ASA III/IV classification increased ACT for THA by 3.76 minutes (P<.001) and increased SCT for THA by 6.33 minutes after controlling for surgeon and location (P=.008). General anesthesia use was higher at the AMC for both THA (29.2% vs 7.3%) and TKA (23.8% vs 4.2%). No statistically significant association was observed between either ACT or SCT and anesthetic type (neuraxial or general) after adjusting for surgeon and location (all P>.05).</p><p><strong>Conclusions: </strong>We observed lower ACT and SCT at the CH for both TKA and THA after controlling for the surgeon of record and ASA classification. These findings underscore the efficiency advantages of performing primary joint replacements at the CH, showcasing an average reduction of 16 minutes in SCT and 4 minutes in ACT per case. Overall, establishing more accurate benchmarks to improve the prediction of surgical duration for THA and TKA in different perioperative environments can increase the reliability of surgical duration predictions and optimize scheduling. Future studies with study populations at multiple community hospitals and academic medical centers are needed before extrapolating these findings.</p>","PeriodicalId":73557,"journal":{"name":"JMIR perioperative medicine","volume":"7 ","pages":"e45126"},"PeriodicalIF":0.0000,"publicationDate":"2024-02-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10928520/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR perioperative medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/45126","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Osteoarthritis is a significant cause of disability, resulting in increased joint replacement surgeries and health care costs. Establishing benchmarks that more accurately predict surgical duration could help to decrease costs, maximize efficiency, and improve patient experience. We compared the anesthesia-controlled time (ACT) and surgery-controlled time (SCT) of primary total knee (TKA) and total hip arthroplasties (THA) between an academic medical center (AMC) and a community hospital (CH) for 2 orthopedic surgeons.
Objective: This study aims to validate and compare benchmarking times for ACT and SCT in a single patient population at both an AMC and a CH.
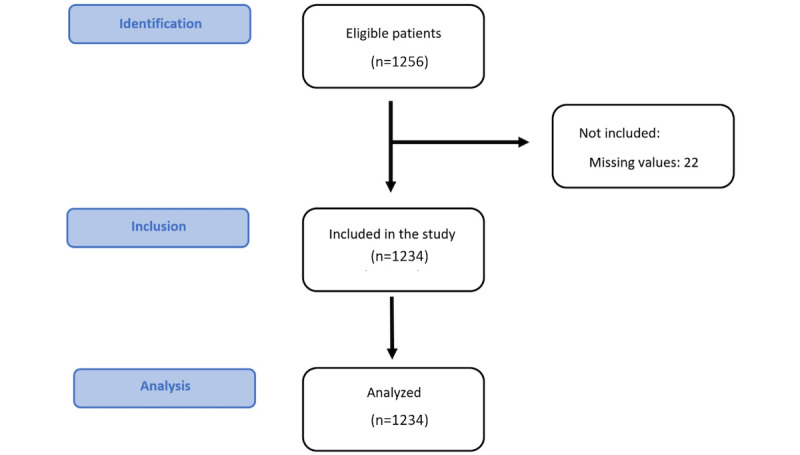
Methods: This retrospective 2-center observational cohort study was conducted at the University of Colorado Hospital (AMC) and UCHealth Broomfield Hospital (CH). Cases with current procedural terminology codes for THA and TKA between January 1, 2019, and December 31, 2020, were assessed. Cases with missing data were excluded. The primary outcomes were ACT and SCT. Primary outcomes were tested for association with covariates of interest. The primary covariate of interest was the location of the procedure (CH vs AMC); secondary covariates of interest included the American Society of Anesthesiologists (ASA) classification and anesthetic type. Linear regression models were used to assess the relationships.
Results: Two surgeons performed 1256 cases at the AMC and CH. A total of 10 THA cases and 12 TKA cases were excluded due to missing data. After controlling for surgeon, the ACT was greater at the AMC for THA by 3.77 minutes and for TKA by 3.58 minutes (P<.001). SCT was greater at the AMC for THA by 11.14 minutes and for TKA by 14.04 minutes (P<.001). ASA III/IV classification increased ACT for THA by 3.76 minutes (P<.001) and increased SCT for THA by 6.33 minutes after controlling for surgeon and location (P=.008). General anesthesia use was higher at the AMC for both THA (29.2% vs 7.3%) and TKA (23.8% vs 4.2%). No statistically significant association was observed between either ACT or SCT and anesthetic type (neuraxial or general) after adjusting for surgeon and location (all P>.05).
Conclusions: We observed lower ACT and SCT at the CH for both TKA and THA after controlling for the surgeon of record and ASA classification. These findings underscore the efficiency advantages of performing primary joint replacements at the CH, showcasing an average reduction of 16 minutes in SCT and 4 minutes in ACT per case. Overall, establishing more accurate benchmarks to improve the prediction of surgical duration for THA and TKA in different perioperative environments can increase the reliability of surgical duration predictions and optimize scheduling. Future studies with study populations at multiple community hospitals and academic medical centers are needed before extrapolating these findings.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
