Real-World Impact of Blood Pressure Control in Patients With Apparent Treatment-Resistant or Difficult-to-Control Hypertension and Stages 3 and 4 Chronic Kidney Disease.
George Bakris, Cindy Chen, Alicia K Campbell, Veronica Ashton, Lloyd Haskell, Mukul Singhal
{"title":"Real-World Impact of Blood Pressure Control in Patients With Apparent Treatment-Resistant or Difficult-to-Control Hypertension and Stages 3 and 4 Chronic Kidney Disease.","authors":"George Bakris, Cindy Chen, Alicia K Campbell, Veronica Ashton, Lloyd Haskell, Mukul Singhal","doi":"10.1093/ajh/hpae020","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic kidney disease (CKD) is a common comorbidity in patients with apparent treatment-resistant hypertension (aTRH). We assessed clinical outcomes, healthcare resource utilization events, and costs in patients with aTRH or difficult-to-control hypertension and stage 3-4 CKD with uncontrolled vs. controlled BP.</p><p><strong>Methods: </strong>This retrospective cohort study used linked IQVIA Ambulatory EMR-US and IQVIA PharMetrics Plus claims databases. Adult patients had claims for ≥3 antihypertensive medication classes within 30 days between 01/01/2015 and 06/30/2021, 2 office BP measures recorded 1-90 days apart, ≥1 claim with ICD-9/10-CM diagnosis codes for CKD 3/4, and ≥1 year of continuous enrollment. Baseline BP was defined as uncontrolled (≥130/80 mm Hg) or controlled (<130/80 mm Hg) BP. Outcomes included risk of major adverse cardiovascular events plus (MACE+; stroke, myocardial infarction, heart failure hospitalization), end-stage renal disease (ESRD), healthcare resource utilization events, and costs during follow-up.</p><p><strong>Results: </strong>Of 3,966 patients with stage 3-4 CKD using ≥3 antihypertensive medications, 2,479 had uncontrolled BP and 1,487 had controlled BP. After adjusting for baseline differences, patients with uncontrolled vs. controlled BP had a higher risk of MACE+ (HR [95% CI]: 1.18 [1.03-1.36]), ESRD (1.85 [1.44-2.39]), inpatient hospitalization (rate ratio [95% CI]: 1.35 [1.28-1.43]), and outpatient visits (1.12 [1.11-1.12]) and incurred higher total medical and pharmacy costs (mean difference [95% CI]: $10,055 [$6,741-$13,646] per patient per year).</p><p><strong>Conclusions: </strong>Patients with aTRH and stage 3-4 CKD and uncontrolled BP despite treatment with ≥3 antihypertensive classes had an increased risk of MACE+ and ESRD and incurred greater healthcare resource utilization and medical expenditures compared with patients taking ≥3 antihypertensive classes with controlled BP.</p>","PeriodicalId":7578,"journal":{"name":"American Journal of Hypertension","volume":" ","pages":"438-446"},"PeriodicalIF":3.1000,"publicationDate":"2024-05-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11094384/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hypertension","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ajh/hpae020","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Chronic kidney disease (CKD) is a common comorbidity in patients with apparent treatment-resistant hypertension (aTRH). We assessed clinical outcomes, healthcare resource utilization events, and costs in patients with aTRH or difficult-to-control hypertension and stage 3-4 CKD with uncontrolled vs. controlled BP.
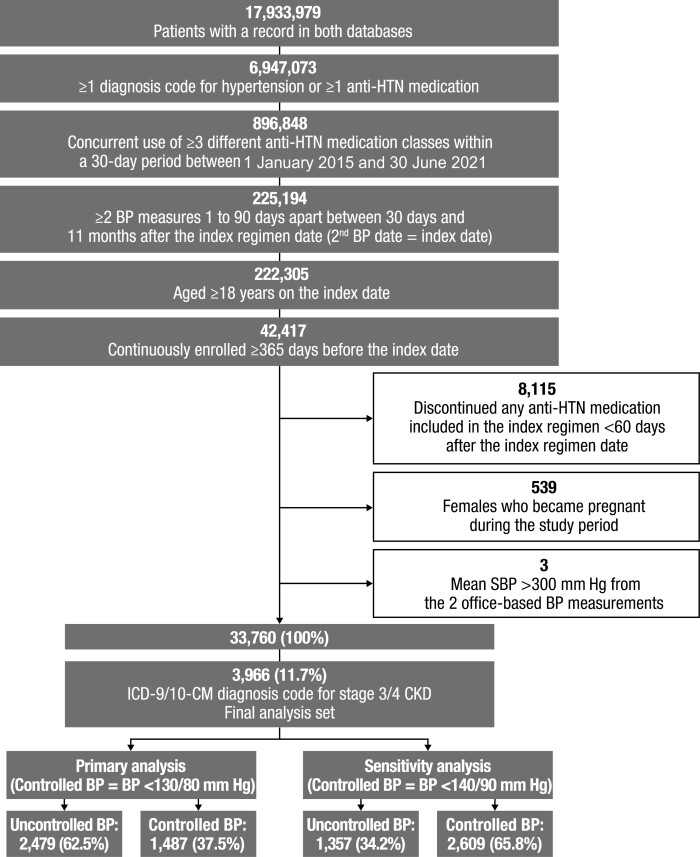
Methods: This retrospective cohort study used linked IQVIA Ambulatory EMR-US and IQVIA PharMetrics Plus claims databases. Adult patients had claims for ≥3 antihypertensive medication classes within 30 days between 01/01/2015 and 06/30/2021, 2 office BP measures recorded 1-90 days apart, ≥1 claim with ICD-9/10-CM diagnosis codes for CKD 3/4, and ≥1 year of continuous enrollment. Baseline BP was defined as uncontrolled (≥130/80 mm Hg) or controlled (<130/80 mm Hg) BP. Outcomes included risk of major adverse cardiovascular events plus (MACE+; stroke, myocardial infarction, heart failure hospitalization), end-stage renal disease (ESRD), healthcare resource utilization events, and costs during follow-up.
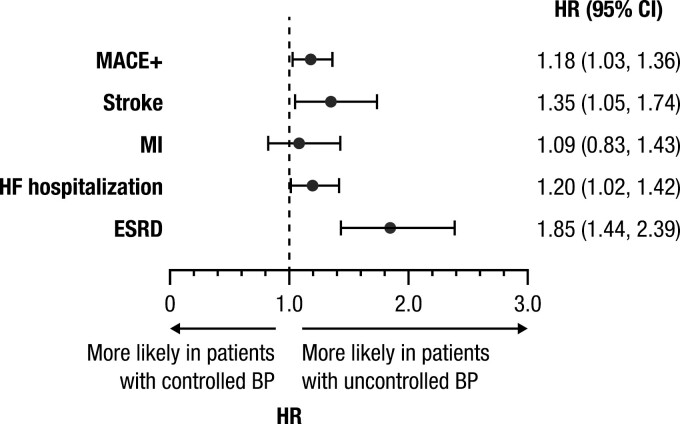
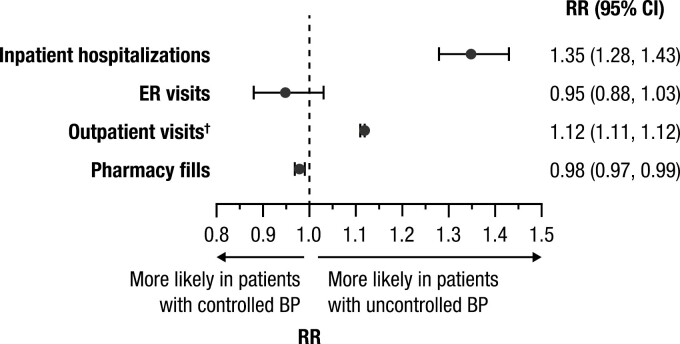
Results: Of 3,966 patients with stage 3-4 CKD using ≥3 antihypertensive medications, 2,479 had uncontrolled BP and 1,487 had controlled BP. After adjusting for baseline differences, patients with uncontrolled vs. controlled BP had a higher risk of MACE+ (HR [95% CI]: 1.18 [1.03-1.36]), ESRD (1.85 [1.44-2.39]), inpatient hospitalization (rate ratio [95% CI]: 1.35 [1.28-1.43]), and outpatient visits (1.12 [1.11-1.12]) and incurred higher total medical and pharmacy costs (mean difference [95% CI]: $10,055 [$6,741-$13,646] per patient per year).
Conclusions: Patients with aTRH and stage 3-4 CKD and uncontrolled BP despite treatment with ≥3 antihypertensive classes had an increased risk of MACE+ and ESRD and incurred greater healthcare resource utilization and medical expenditures compared with patients taking ≥3 antihypertensive classes with controlled BP.
期刊介绍:
The American Journal of Hypertension is a monthly, peer-reviewed journal that provides a forum for scientific inquiry of the highest standards in the field of hypertension and related cardiovascular disease. The journal publishes high-quality original research and review articles on basic sciences, molecular biology, clinical and experimental hypertension, cardiology, epidemiology, pediatric hypertension, endocrinology, neurophysiology, and nephrology.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
