{"title":"Development and Feasibility of an Adolescent Dancer Screen.","authors":"Kynaston Schultz, Kathleen Sun Worrall, Zoe Tawa, Joanna Binney, Jessica Boyle, Laurel Daniels Abbruzzese","doi":"10.26603/001c.92902","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adolescent dancers are at high risk for injuries due to the physical demands of dance training and the physiological changes that occur during adolescence. Though studies report high injury rates, there are few standardized screening tools available for adolescent dancers.</p><p><strong>Hypothesis/purpose: </strong>To develop and describe a standardized, feasible, evidence-based, and clinically relevant screen for adolescent dancers.</p><p><strong>Study design: </strong>Descriptive Epidemiology Study.</p><p><strong>Methods: </strong>Dancers at two suburban pre-professional dance studios, in two cohorts, participated in the Columbia Adolescent Dancer Screen (CADS) that includes dance injury history, health questionnaires (EAT-26, SF-36, DFOS), aerobic capacity, range of motion, strength, balance/orthopedic special tests, and dance technique. Participants were asked to complete a weekly injury surveillance questionnaire derived from the Dance-Specific Oslo Sports Trauma Research Centre Questionnaire on Health Problems for 14 weeks following the screening. Feasibility was assessed using process and content analysis in four areas: practicality, demand, implementation, and adaptation.</p><p><strong>Results: </strong>Descriptive data were collected from 32 female dancers aged 11-17 with cohort one averaging 18.57 dance hours per week and cohort two averaging 10.6 dance hours per week. The screen was practical, able to screen seven to eight dancers per hour utilizing nine assessors and requiring a one-hour commitment from dancers. Cost and space requirements were considered and kept to a minimum while utilizing portable equipment. All screening slots were filled with all dancers agreeing to follow-up injury surveillance, indicating high demand. The screen was implemented with two cohorts with revisions to improve efficiency applied for the second cohort.</p><p><strong>Conclusion: </strong>The CADS is a feasible screening tool for adolescent dancers that overcomes barriers by being pragmatic, evidence-based, and efficient. Screening can be implemented to obtain baseline values, inform wellness recommendations, and establish relationships with medical professionals.</p><p><strong>Level of evidence: </strong>Level 3b.</p>","PeriodicalId":47892,"journal":{"name":"International Journal of Sports Physical Therapy","volume":"19 3","pages":"301-315"},"PeriodicalIF":2.1000,"publicationDate":"2024-03-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10909306/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Sports Physical Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.26603/001c.92902","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SPORT SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Adolescent dancers are at high risk for injuries due to the physical demands of dance training and the physiological changes that occur during adolescence. Though studies report high injury rates, there are few standardized screening tools available for adolescent dancers.
Hypothesis/purpose: To develop and describe a standardized, feasible, evidence-based, and clinically relevant screen for adolescent dancers.
Study design: Descriptive Epidemiology Study.
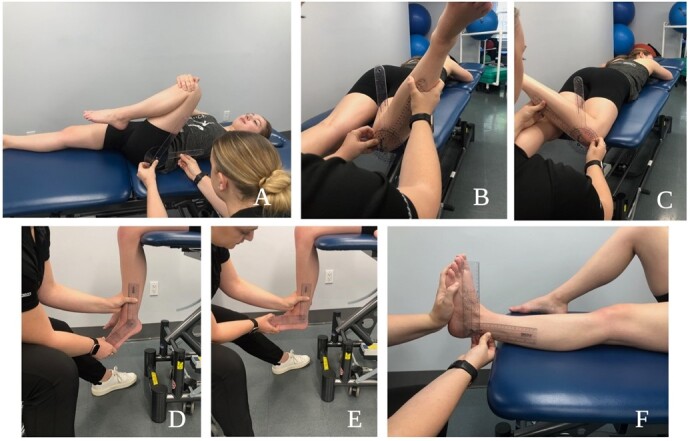
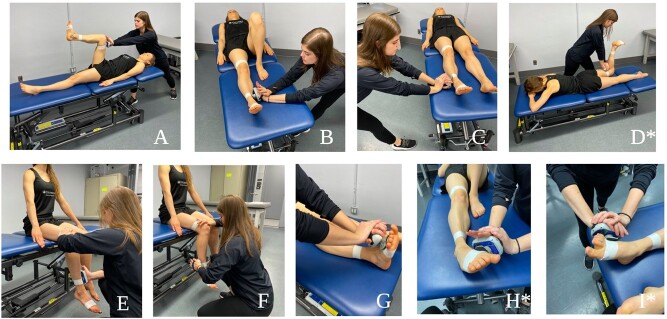
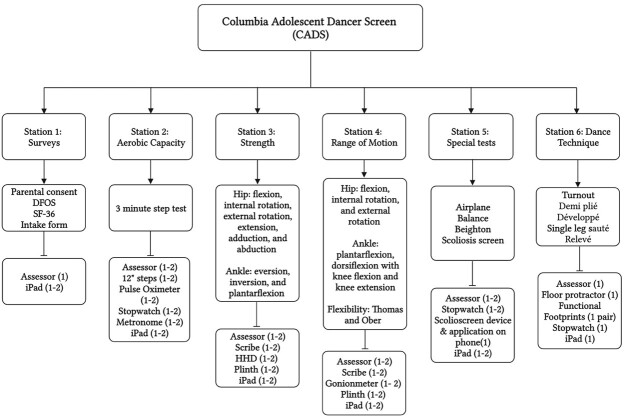
Methods: Dancers at two suburban pre-professional dance studios, in two cohorts, participated in the Columbia Adolescent Dancer Screen (CADS) that includes dance injury history, health questionnaires (EAT-26, SF-36, DFOS), aerobic capacity, range of motion, strength, balance/orthopedic special tests, and dance technique. Participants were asked to complete a weekly injury surveillance questionnaire derived from the Dance-Specific Oslo Sports Trauma Research Centre Questionnaire on Health Problems for 14 weeks following the screening. Feasibility was assessed using process and content analysis in four areas: practicality, demand, implementation, and adaptation.
Results: Descriptive data were collected from 32 female dancers aged 11-17 with cohort one averaging 18.57 dance hours per week and cohort two averaging 10.6 dance hours per week. The screen was practical, able to screen seven to eight dancers per hour utilizing nine assessors and requiring a one-hour commitment from dancers. Cost and space requirements were considered and kept to a minimum while utilizing portable equipment. All screening slots were filled with all dancers agreeing to follow-up injury surveillance, indicating high demand. The screen was implemented with two cohorts with revisions to improve efficiency applied for the second cohort.
Conclusion: The CADS is a feasible screening tool for adolescent dancers that overcomes barriers by being pragmatic, evidence-based, and efficient. Screening can be implemented to obtain baseline values, inform wellness recommendations, and establish relationships with medical professionals.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
