Neuraxial clonidine is not associated with lower post-cesarean opioid consumption or pain scores in parturients on chronic buprenorphine therapy: a retrospective cohort study.
Michael G Taylor, Jeanette R Bauchat, Laura L Sorabella, Jonathan P Wanderer, Xiaoke Feng, Matthew S Shotwell, Holly B Ende
{"title":"Neuraxial clonidine is not associated with lower post-cesarean opioid consumption or pain scores in parturients on chronic buprenorphine therapy: a retrospective cohort study.","authors":"Michael G Taylor, Jeanette R Bauchat, Laura L Sorabella, Jonathan P Wanderer, Xiaoke Feng, Matthew S Shotwell, Holly B Ende","doi":"10.1007/s00540-024-03314-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Adequate post-cesarean delivery analgesia can be difficult to achieve for women diagnosed with opioid use disorder receiving buprenorphine. We sought to determine if neuraxial clonidine administration is associated with decreased opioid consumption and pain scores following cesarean delivery in women receiving chronic buprenorphine therapy.</p><p><strong>Methods: </strong>This was a retrospective cohort study at a tertiary care teaching hospital of women undergoing cesarean delivery with or without neuraxial clonidine administration while receiving chronic buprenorphine. The primary outcome was opioid consumption (in morphine milligram equivalents) 0-6 h following cesarean delivery. Secondary outcomes included opioid consumption 0-24 h post-cesarean, median postoperative pain scores 0-24 h, and rates of intraoperative anesthetic supplementation. Multivariable analysis evaluating the adjusted effects of neuraxial clonidine on outcomes was conducted using linear regression, proportional odds model, and logistic regression separately.</p><p><strong>Results: </strong>196 women met inclusion criteria, of which 145 (74%) received neuraxial clonidine while 51 (26%) did not. In univariate analysis, there was no significant difference in opioid consumption 0-6 h post-cesarean delivery between the clonidine (8 [IQR 0, 15]) and control (1 [IQR 0, 8]) groups (P = 0.14). After adjusting for potential confounders, there remained no significant association with neuraxial clonidine administration 0-6 h (Difference in means 2.77, 95% CI [- 0.89 to 6.44], P = 0.14) or 0-24 h (Difference in means 8.56, 95% CI [- 16.99 to 34.11], P = 0.51).</p><p><strong>Conclusion: </strong>In parturients receiving chronic buprenorphine therapy at the time of cesarean delivery, neuraxial clonidine administration was not associated with decreased postoperative opioid consumption, median pain scores, or the need for intraoperative supplementation.</p>","PeriodicalId":14997,"journal":{"name":"Journal of Anesthesia","volume":" ","pages":"339-346"},"PeriodicalIF":2.7000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Anesthesia","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00540-024-03314-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/10 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Adequate post-cesarean delivery analgesia can be difficult to achieve for women diagnosed with opioid use disorder receiving buprenorphine. We sought to determine if neuraxial clonidine administration is associated with decreased opioid consumption and pain scores following cesarean delivery in women receiving chronic buprenorphine therapy.
Methods: This was a retrospective cohort study at a tertiary care teaching hospital of women undergoing cesarean delivery with or without neuraxial clonidine administration while receiving chronic buprenorphine. The primary outcome was opioid consumption (in morphine milligram equivalents) 0-6 h following cesarean delivery. Secondary outcomes included opioid consumption 0-24 h post-cesarean, median postoperative pain scores 0-24 h, and rates of intraoperative anesthetic supplementation. Multivariable analysis evaluating the adjusted effects of neuraxial clonidine on outcomes was conducted using linear regression, proportional odds model, and logistic regression separately.
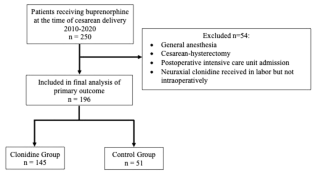
Results: 196 women met inclusion criteria, of which 145 (74%) received neuraxial clonidine while 51 (26%) did not. In univariate analysis, there was no significant difference in opioid consumption 0-6 h post-cesarean delivery between the clonidine (8 [IQR 0, 15]) and control (1 [IQR 0, 8]) groups (P = 0.14). After adjusting for potential confounders, there remained no significant association with neuraxial clonidine administration 0-6 h (Difference in means 2.77, 95% CI [- 0.89 to 6.44], P = 0.14) or 0-24 h (Difference in means 8.56, 95% CI [- 16.99 to 34.11], P = 0.51).
Conclusion: In parturients receiving chronic buprenorphine therapy at the time of cesarean delivery, neuraxial clonidine administration was not associated with decreased postoperative opioid consumption, median pain scores, or the need for intraoperative supplementation.
期刊介绍:
The Journal of Anesthesia is the official journal of the Japanese Society of Anesthesiologists. This journal publishes original articles, review articles, special articles, clinical reports, short communications, letters to the editor, and book and multimedia reviews. The editors welcome the submission of manuscripts devoted to anesthesia and related topics from any country of the world. Membership in the Society is not a prerequisite.
The Journal of Anesthesia (JA) welcomes case reports that show unique cases in perioperative medicine, intensive care, emergency medicine, and pain management.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
