Ahmad Beyh, Samuel E Rasche, Alexander Leff, Dominic Ffytche, Semir Zeki
{"title":"A clinico-anatomical dissection of the magnocellular and parvocellular pathways in a patient with the Riddoch syndrome.","authors":"Ahmad Beyh, Samuel E Rasche, Alexander Leff, Dominic Ffytche, Semir Zeki","doi":"10.1007/s00429-024-02774-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Key message: </strong>The Riddoch syndrome is thought to be caused by damage to the primary visual cortex (V1), usually following a vascular event. This study shows that damage to the anatomical input to V1, i.e., the optic radiations, can result in selective visual deficits that mimic the Riddoch syndrome. The results also highlight the differential susceptibility of the magnocellular and parvocellular visual systems to injury. Overall, this study offers new insights that will improve our understanding of the impact of brain injury and neurosurgery on the visual pathways. The Riddoch syndrome, characterised by the ability to perceive, consciously, moving visual stimuli but not static ones, has been associated with lesions of primary visual cortex (V1). We present here the case of patient YL who, after a tumour resection surgery that spared his V1, nevertheless showed symptoms of the Riddoch syndrome. Based on our testing, we postulated that the magnocellular (M) and parvocellular (P) inputs to his V1 may be differentially affected. In a first experiment, YL was presented with static and moving checkerboards in his blind field while undergoing multimodal magnetic resonance imaging (MRI), including structural, functional, and diffusion, acquired at 3 T. In a second experiment, we assessed YL's neural responses to M and P visual stimuli using psychophysics and high-resolution fMRI acquired at 7 T. YL's optic radiations were partially damaged but not severed. We found extensive activity in his visual cortex for moving, but not static, visual stimuli, while our psychophysical tests revealed that only low-spatial frequency moving checkerboards were perceived. High-resolution fMRI revealed strong responses in YL's V1 to M stimuli and very weak ones to P stimuli, indicating a functional P lesion affecting V1. In addition, YL frequently reported seeing moving stimuli and discriminating their direction of motion in the absence of visual stimulation, suggesting that he was experiencing visual hallucinations. Overall, this study highlights the possibility of a selective loss of P inputs to V1 resulting in the Riddoch syndrome and in hallucinations of visual motion.</p>","PeriodicalId":9145,"journal":{"name":"Brain Structure & Function","volume":" ","pages":"937-946"},"PeriodicalIF":2.9000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11004049/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain Structure & Function","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00429-024-02774-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/16 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANATOMY & MORPHOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
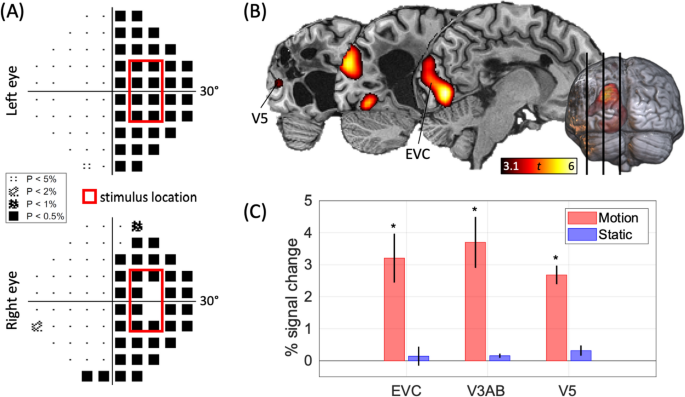
Key message: The Riddoch syndrome is thought to be caused by damage to the primary visual cortex (V1), usually following a vascular event. This study shows that damage to the anatomical input to V1, i.e., the optic radiations, can result in selective visual deficits that mimic the Riddoch syndrome. The results also highlight the differential susceptibility of the magnocellular and parvocellular visual systems to injury. Overall, this study offers new insights that will improve our understanding of the impact of brain injury and neurosurgery on the visual pathways. The Riddoch syndrome, characterised by the ability to perceive, consciously, moving visual stimuli but not static ones, has been associated with lesions of primary visual cortex (V1). We present here the case of patient YL who, after a tumour resection surgery that spared his V1, nevertheless showed symptoms of the Riddoch syndrome. Based on our testing, we postulated that the magnocellular (M) and parvocellular (P) inputs to his V1 may be differentially affected. In a first experiment, YL was presented with static and moving checkerboards in his blind field while undergoing multimodal magnetic resonance imaging (MRI), including structural, functional, and diffusion, acquired at 3 T. In a second experiment, we assessed YL's neural responses to M and P visual stimuli using psychophysics and high-resolution fMRI acquired at 7 T. YL's optic radiations were partially damaged but not severed. We found extensive activity in his visual cortex for moving, but not static, visual stimuli, while our psychophysical tests revealed that only low-spatial frequency moving checkerboards were perceived. High-resolution fMRI revealed strong responses in YL's V1 to M stimuli and very weak ones to P stimuli, indicating a functional P lesion affecting V1. In addition, YL frequently reported seeing moving stimuli and discriminating their direction of motion in the absence of visual stimulation, suggesting that he was experiencing visual hallucinations. Overall, this study highlights the possibility of a selective loss of P inputs to V1 resulting in the Riddoch syndrome and in hallucinations of visual motion.
期刊介绍:
Brain Structure & Function publishes research that provides insight into brain structure−function relationships. Studies published here integrate data spanning from molecular, cellular, developmental, and systems architecture to the neuroanatomy of behavior and cognitive functions. Manuscripts with focus on the spinal cord or the peripheral nervous system are not accepted for publication. Manuscripts with focus on diseases, animal models of diseases, or disease-related mechanisms are only considered for publication, if the findings provide novel insight into the organization and mechanisms of normal brain structure and function.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
