Juliana Damas, Catarina Marouço, Rui Barata, Tiago Assis Pereira, Nuno Moreira Fonseca, David Navarro, Mário Góis, Helena Viana, João Sousa, Heidi Gruner, Cristina Jorge
{"title":"IgA Nephropathy and Remitting Seronegative Symmetrical Synovitis with Pitting Edema (RS3PE): A Case Report","authors":"Juliana Damas, Catarina Marouço, Rui Barata, Tiago Assis Pereira, Nuno Moreira Fonseca, David Navarro, Mário Góis, Helena Viana, João Sousa, Heidi Gruner, Cristina Jorge","doi":"10.1007/s42399-024-01663-9","DOIUrl":null,"url":null,"abstract":"<p>IgA nephropathy (IgAN) remains the most frequent glomerular disease worldwide, with a broad spectrum of clinical and histological presentations. It has been associated with many secondary causes. The remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome is an autoimmune disorder characterized by swelling in the extremities and negative autoimmune serological tests. The primary treatment for this condition involves the use of immunosuppressive therapy. Although several triggers have been identified, the exact cause of this condition is still unknown. We report a case of a 53-year-old man who presented with acute exacerbation of chronic kidney disease, whose etiological study revealed advanced IgAN, associated with pleural and pericardial effusions. Even with volume optimization and dialysis intensification, the pericardial effusion worsened, despite the resolving pleural effusion. Upper arm arthralgias were developed afterward. An extensive study ruled out other causes and the hypothesis of RS3PE syndrome was considered. Glucocorticoid (GC) therapy was instituted for 6 months with clinical improvement and no recurrence at 2 years follow-up. The complexity of this case shows the importance of considering a wider diagnosis for the complaints of arthralgias and volume overload, reinforcing the importance of clinical awareness for other concurrent conditions, whose treatment may be lifesaving.</p>","PeriodicalId":21944,"journal":{"name":"SN Comprehensive Clinical Medicine","volume":"19 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-03-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"SN Comprehensive Clinical Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s42399-024-01663-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
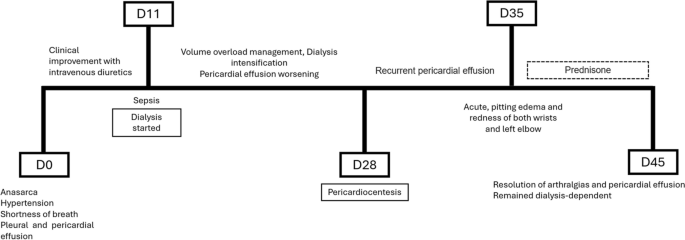
IgA nephropathy (IgAN) remains the most frequent glomerular disease worldwide, with a broad spectrum of clinical and histological presentations. It has been associated with many secondary causes. The remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome is an autoimmune disorder characterized by swelling in the extremities and negative autoimmune serological tests. The primary treatment for this condition involves the use of immunosuppressive therapy. Although several triggers have been identified, the exact cause of this condition is still unknown. We report a case of a 53-year-old man who presented with acute exacerbation of chronic kidney disease, whose etiological study revealed advanced IgAN, associated with pleural and pericardial effusions. Even with volume optimization and dialysis intensification, the pericardial effusion worsened, despite the resolving pleural effusion. Upper arm arthralgias were developed afterward. An extensive study ruled out other causes and the hypothesis of RS3PE syndrome was considered. Glucocorticoid (GC) therapy was instituted for 6 months with clinical improvement and no recurrence at 2 years follow-up. The complexity of this case shows the importance of considering a wider diagnosis for the complaints of arthralgias and volume overload, reinforcing the importance of clinical awareness for other concurrent conditions, whose treatment may be lifesaving.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
