Wilfried Gwinner, Swapneel Anaokar, Martin Blogg, Birgit Hermann, Carola Del Pilar Repetur, Mario Schiffer
{"title":"Long-Term Outcomes with Prolonged-Release Tacrolimus in Kidney Transplantation: A Retrospective Real-World Data Analysis.","authors":"Wilfried Gwinner, Swapneel Anaokar, Martin Blogg, Birgit Hermann, Carola Del Pilar Repetur, Mario Schiffer","doi":"10.12659/AOT.942167","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Long-term real-world outcomes data for kidney transplant recipients (KTRs) converting from immediate-release tacrolimus (IRT) to prolonged-release tacrolimus (PRT) are limited. MATERIAL AND METHODS A retrospective, non-interventional review of adult KTRs treated with PRT for ≥1 month was conducted in Germany. Data were extracted from time of transplant (2008-2014) to 2018. Primary composite endpoints (graft loss, biopsy-confirmed acute rejection, graft dysfunction) and secondary endpoints (all-cause mortality, kidney function course, and tacrolimus dose/trough levels) were analyzed for sub-cohorts: de novo PRT, early conversion from IRT (within 6 months post-transplant), and late conversion (7 months to 3 years). RESULTS Analysis included 163 patients (101 de novo, 12 early converters, and 50 late converters). The overall Kaplan-Meier estimate of freedom from efficacy failure through 5 years was 0.537, (95% confidence interval (CI) 0.455-0.612) (de novo: 0.512 [0.407-0.608]; early converters: 0.500 [0.208-0.736]; late converters: 0.594 [0.443-0.717]). The overall survival rate was 0.925 (95% CI 0.872-0.957) (de novo: 0.900 [0.823-0.945]; early converters: 0.917 [0.539-0.988]; late converters: 0.977 [0.846-0.997]). During follow-up, there was a gradual reduction in tacrolimus dose and trough levels; kidney function remained stable in all cohorts. Multivariable analysis found re-transplantation, organ donor quality, best estimated glomerular filtration rate 8-12 weeks after transplant, and treatment center (between-center differences in age, sex, donor status/quality) were significantly associated with efficacy failure. CONCLUSIONS There was no difference in long-term survival profiles between KTRs who received PRT de novo vs those who converted from IRT, with 5-year survival remaining high in both groups.</p>","PeriodicalId":7935,"journal":{"name":"Annals of Transplantation","volume":"29 ","pages":"e942167"},"PeriodicalIF":1.4000,"publicationDate":"2024-03-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10960500/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Transplantation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.12659/AOT.942167","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
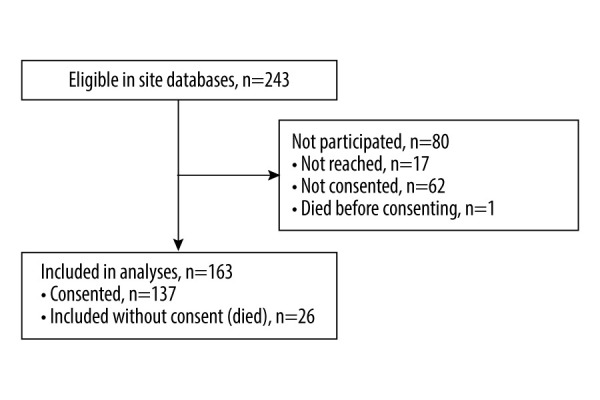
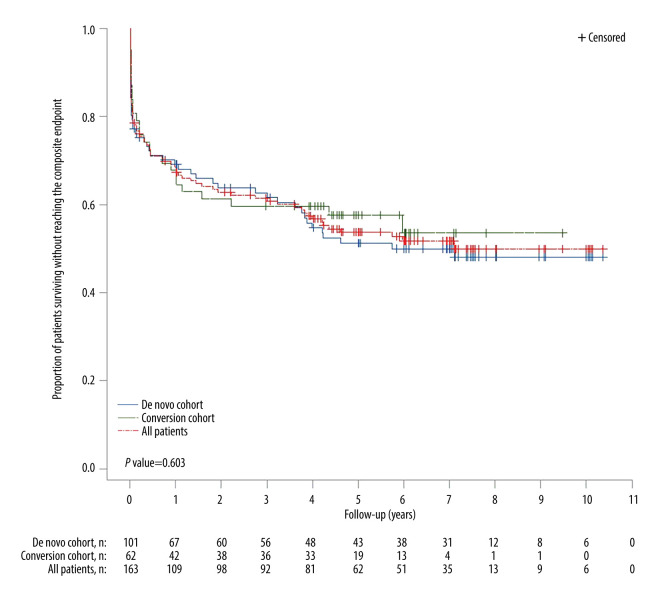
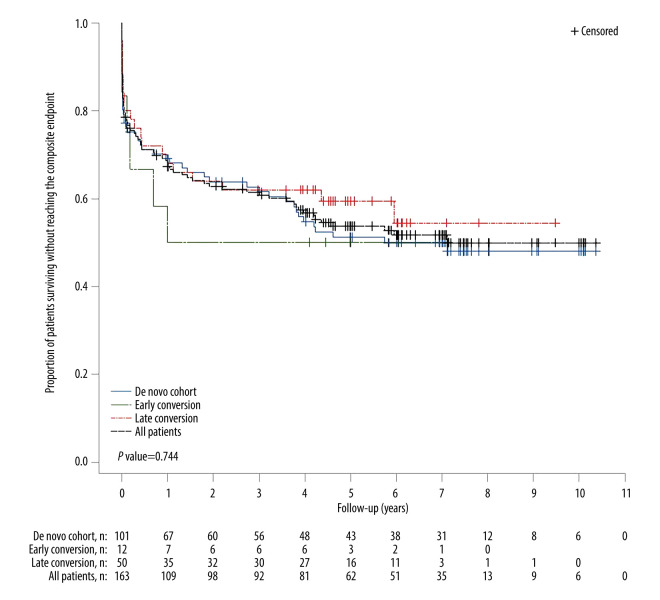
BACKGROUND Long-term real-world outcomes data for kidney transplant recipients (KTRs) converting from immediate-release tacrolimus (IRT) to prolonged-release tacrolimus (PRT) are limited. MATERIAL AND METHODS A retrospective, non-interventional review of adult KTRs treated with PRT for ≥1 month was conducted in Germany. Data were extracted from time of transplant (2008-2014) to 2018. Primary composite endpoints (graft loss, biopsy-confirmed acute rejection, graft dysfunction) and secondary endpoints (all-cause mortality, kidney function course, and tacrolimus dose/trough levels) were analyzed for sub-cohorts: de novo PRT, early conversion from IRT (within 6 months post-transplant), and late conversion (7 months to 3 years). RESULTS Analysis included 163 patients (101 de novo, 12 early converters, and 50 late converters). The overall Kaplan-Meier estimate of freedom from efficacy failure through 5 years was 0.537, (95% confidence interval (CI) 0.455-0.612) (de novo: 0.512 [0.407-0.608]; early converters: 0.500 [0.208-0.736]; late converters: 0.594 [0.443-0.717]). The overall survival rate was 0.925 (95% CI 0.872-0.957) (de novo: 0.900 [0.823-0.945]; early converters: 0.917 [0.539-0.988]; late converters: 0.977 [0.846-0.997]). During follow-up, there was a gradual reduction in tacrolimus dose and trough levels; kidney function remained stable in all cohorts. Multivariable analysis found re-transplantation, organ donor quality, best estimated glomerular filtration rate 8-12 weeks after transplant, and treatment center (between-center differences in age, sex, donor status/quality) were significantly associated with efficacy failure. CONCLUSIONS There was no difference in long-term survival profiles between KTRs who received PRT de novo vs those who converted from IRT, with 5-year survival remaining high in both groups.
期刊介绍:
Annals of Transplantation is one of the fast-developing journals open to all scientists and fields of transplant medicine and related research. The journal is published quarterly and provides extensive coverage of the most important advances in transplantation.
Using an electronic on-line submission and peer review tracking system, Annals of Transplantation is committed to rapid review and publication. The average time to first decision is around 3-4 weeks. Time to publication of accepted manuscripts continues to be shortened, with the Editorial team committed to a goal of 3 months from acceptance to publication.
Expert reseachers and clinicians from around the world contribute original Articles, Review Papers, Case Reports and Special Reports in every pertinent specialty, providing a lot of arguments for discussion of exciting developments and controversies in the field.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
