Jan Puetzler, Marc Hofschneider, Georg Gosheger, Christoph Theil, Martin Schulze, Jan Schwarze, Raphael Koch, Burkhard Moellenbeck
{"title":"Evaluation of time to reimplantation as a risk factor in two-stage revision with static spacers for periprosthetic knee joint infection.","authors":"Jan Puetzler, Marc Hofschneider, Georg Gosheger, Christoph Theil, Martin Schulze, Jan Schwarze, Raphael Koch, Burkhard Moellenbeck","doi":"10.1186/s10195-024-00745-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>We investigated the time to reimplantation (TTR) during two-stage revision using static spacers with regard to treatment success and function in patients with chronic periprosthetic joint infection (PJI) of the knee.</p><p><strong>Methods: </strong>163 patients (median age 72 years, 72 women) who underwent two-stage exchange for chronic knee PJI between 2012 and 2020 were retrospectively analyzed (based on the 2011 Musculoskeletal Infection Society criteria). A cutoff TTR for increased risk of reinfection was identified using the maximally selected log-rank statistic. Infection control, aseptic revisions and overall survival were analyzed using Kaplan-Meier survival estimates. Adjustment for confounding factors-the Charlson Comorbidity Index (CCI) and C-reactive protein (CRP)-was done with a Cox proportional hazards model.</p><p><strong>Results: </strong>When TTR exceeded 94 days, the adjusted hazard of reinfection was increased 2.8-fold (95% CI 1.4-5.7; p = 0.0036). The reinfection-free rate was 67% (95% CI 52-79%) after 2 years and 33% (95% CI 11-57%) after 5 years for a longer TTR compared to 89% (95% CI 81-94%) and 80% (95% CI 69-87%) at 2 and 5 years, respectively, for a shorter TTR. Adjusted overall survival and number of aseptic revisions did not differ between the longer TTR and shorter TTR groups. Maximum knee flexion was 90° (IQR 84-100) for a longer TTR and 95° (IQR 90-100) for a shorter TTR (p = 0.0431), with no difference between the groups in Oxford Knee Score. Baseline characteristics were similar (body mass index, age, previous surgeries, microorganisms) for the two groups, except that there was a higher CCI (median 4 vs. 3) and higher CRP (median 3.7 vs 2.6 mg/dl) in the longer TTR group.</p><p><strong>Conclusion: </strong>A long TTR is sometimes unavoidable in clinical practice, but surgeons should be aware of a potentially higher risk of reinfection.</p><p><strong>Level of evidence: </strong>III, retrospective comparative study.</p>","PeriodicalId":48603,"journal":{"name":"Journal of Orthopaedics and Traumatology","volume":"25 1","pages":"15"},"PeriodicalIF":3.7000,"publicationDate":"2024-03-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10963354/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Orthopaedics and Traumatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s10195-024-00745-7","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: We investigated the time to reimplantation (TTR) during two-stage revision using static spacers with regard to treatment success and function in patients with chronic periprosthetic joint infection (PJI) of the knee.
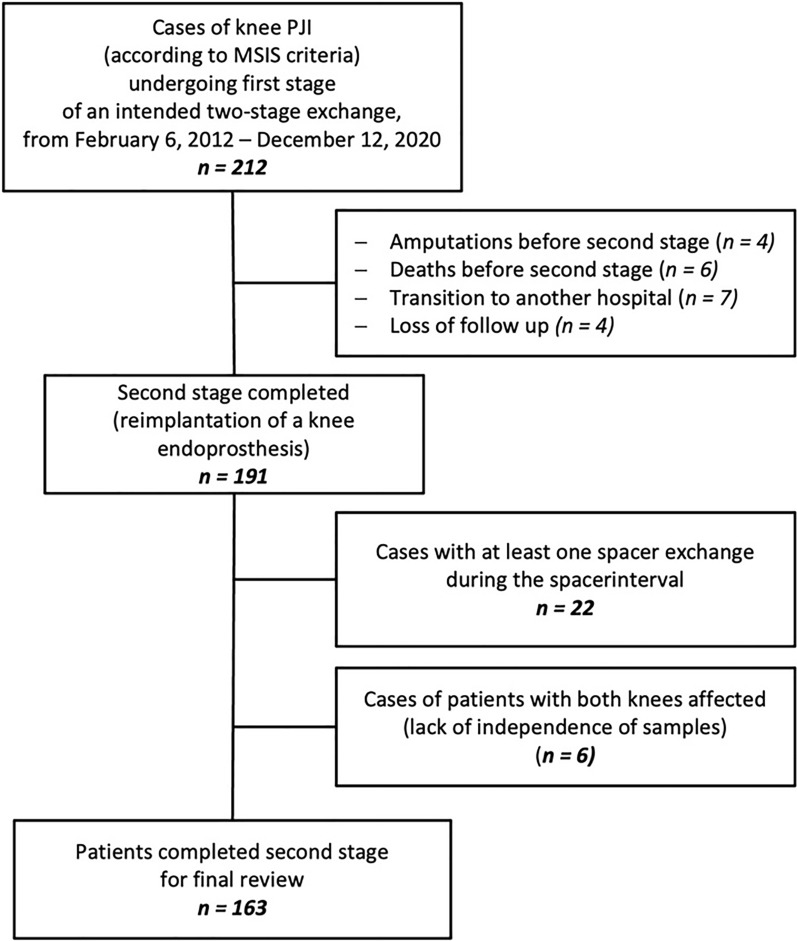
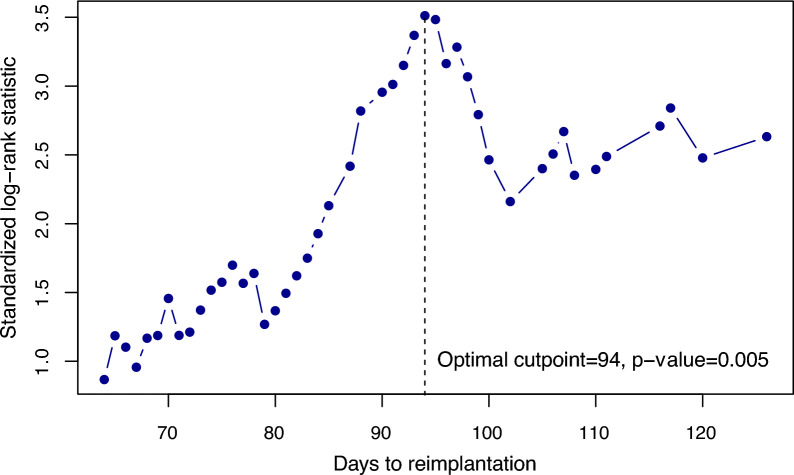
Methods: 163 patients (median age 72 years, 72 women) who underwent two-stage exchange for chronic knee PJI between 2012 and 2020 were retrospectively analyzed (based on the 2011 Musculoskeletal Infection Society criteria). A cutoff TTR for increased risk of reinfection was identified using the maximally selected log-rank statistic. Infection control, aseptic revisions and overall survival were analyzed using Kaplan-Meier survival estimates. Adjustment for confounding factors-the Charlson Comorbidity Index (CCI) and C-reactive protein (CRP)-was done with a Cox proportional hazards model.
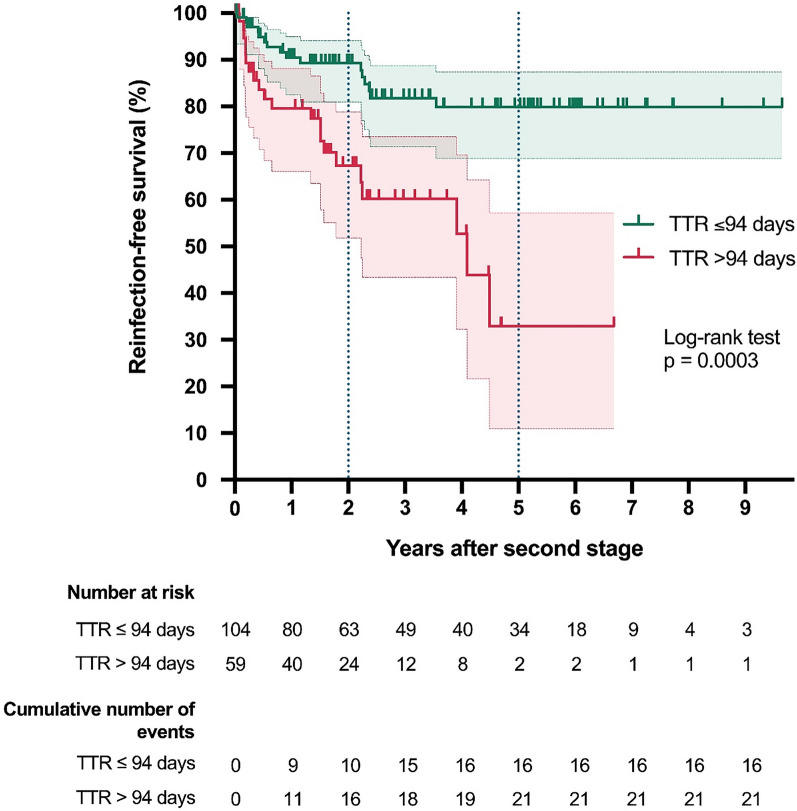
Results: When TTR exceeded 94 days, the adjusted hazard of reinfection was increased 2.8-fold (95% CI 1.4-5.7; p = 0.0036). The reinfection-free rate was 67% (95% CI 52-79%) after 2 years and 33% (95% CI 11-57%) after 5 years for a longer TTR compared to 89% (95% CI 81-94%) and 80% (95% CI 69-87%) at 2 and 5 years, respectively, for a shorter TTR. Adjusted overall survival and number of aseptic revisions did not differ between the longer TTR and shorter TTR groups. Maximum knee flexion was 90° (IQR 84-100) for a longer TTR and 95° (IQR 90-100) for a shorter TTR (p = 0.0431), with no difference between the groups in Oxford Knee Score. Baseline characteristics were similar (body mass index, age, previous surgeries, microorganisms) for the two groups, except that there was a higher CCI (median 4 vs. 3) and higher CRP (median 3.7 vs 2.6 mg/dl) in the longer TTR group.
Conclusion: A long TTR is sometimes unavoidable in clinical practice, but surgeons should be aware of a potentially higher risk of reinfection.
Level of evidence: III, retrospective comparative study.
简介:方法:回顾性分析了2012年至2020年间因慢性膝关节PJI接受两阶段置换术的163例患者(中位年龄72岁,女性72例)(基于2011年肌肉骨骼感染学会标准)。采用最大选择对数秩统计法确定了再感染风险增加的TTR临界值。采用 Kaplan-Meier 存活率估算法分析了感染控制、无菌翻修和总存活率。使用 Cox 比例危险度模型对混杂因素--Charlson 合并症指数(CCI)和 C 反应蛋白(CRP)进行了调整:当 TTR 超过 94 天时,调整后的再感染风险增加了 2.8 倍(95% CI 1.4-5.7;P = 0.0036)。TTR越长,2年后无再感染率为67%(95% CI 52-79%),5年后为33%(95% CI 11-57%);TTR越短,2年后无再感染率为89%(95% CI 81-94%),5年后为80%(95% CI 69-87%)。调整后的总生存率和无菌翻修次数在较长的TTR组和较短的TTR组之间没有差异。TTR较长的患者膝关节最大屈曲度为90°(IQR 84-100),TTR较短的患者膝关节最大屈曲度为95°(IQR 90-100)(p = 0.0431),两组患者的牛津膝关节评分无差异。两组患者的基线特征(体重指数、年龄、既往手术、微生物)相似,但TTR较长组的CCI(中位数为4 vs. 3)和CRP(中位数为3.7 vs. 2.6 mg/dl)较高:结论:在临床实践中,长TTR有时是不可避免的,但外科医生应意识到再感染的潜在风险较高:证据等级:III,回顾性比较研究。
期刊介绍:
The Journal of Orthopaedics and Traumatology, the official open access peer-reviewed journal of the Italian Society of Orthopaedics and Traumatology, publishes original papers reporting basic or clinical research in the field of orthopaedic and traumatologic surgery, as well as systematic reviews, brief communications, case reports and letters to the Editor. Narrative instructional reviews and commentaries to original articles may be commissioned by Editors from eminent colleagues. The Journal of Orthopaedics and Traumatology aims to be an international forum for the communication and exchange of ideas concerning the various aspects of orthopaedics and musculoskeletal trauma.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
