Faizah Shareef, Balambal Bharti, Felipe Garcia-Bigley, Monica Hernandez, Jesse Nodora, Jie Liu, Christian Ramers, Jill Dumbauld Nery, Jessica Marquez, Karina Moyano, Sarah Rojas, Elva Arredondo, Samir Gupta
{"title":"Abnormal Colorectal Cancer Test Follow-Up: A Quality Improvement Initiative at a Federally Qualified Health Center.","authors":"Faizah Shareef, Balambal Bharti, Felipe Garcia-Bigley, Monica Hernandez, Jesse Nodora, Jie Liu, Christian Ramers, Jill Dumbauld Nery, Jessica Marquez, Karina Moyano, Sarah Rojas, Elva Arredondo, Samir Gupta","doi":"10.1177/21501319241242571","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction/objectives: </strong>Colonoscopy completion rates after an abnormal fecal immunochemical test (FIT) are suboptimal, resulting in missed opportunities for early detection and prevention of colorectal cancer. Patient navigation and structured follow-up may improve colonoscopy completion, but implementation of these strategies is not widespread.</p><p><strong>Methods: </strong>We conducted a quality improvement study using a Plan-Do-Study-Act (PDSA) Model to increase colonoscopy completion after abnormal FIT in a large federally qualified health center serving a diverse and low-income population. Intervention components included patient navigation, and a checklist to promote completion of key steps required for abnormal FIT follow-up. Primary outcome was proportion of patients achieving colonoscopy completion within 6 months of abnormal FIT, assessed at baseline for 156 patients pre-intervention, and compared to 208 patients during the intervention period from April 2017 to December 2019. Drop offs at each step in the follow-up process were assessed.</p><p><strong>Results: </strong>Colonoscopy completion improved from 21% among 156 patients with abnormal FIT pre-intervention, to 38% among 208 patients with abnormal FIT during the intervention (<i>P</i> < .001; absolute increase: 17%, 95% CI: 6.9%-25.2%). Among the 130 non-completers during the intervention period, lack of completion was attributable to absence of colonoscopy referral for 7.7%; inability to schedule a pre-colonoscopy specialist visit for 71.5%; failure to complete a pre-colonoscopy visit for 2.3%; the absence of colonoscopy scheduling for 9.2%; failure to show for a scheduled colonoscopy for 9.2%.</p><p><strong>Conclusions: </strong>Patient navigation and structured follow-up appear to improve colonoscopy completion after abnormal FIT. Additional strategies are needed to achieve optimal rates of completion.</p>","PeriodicalId":46723,"journal":{"name":"Journal of Primary Care and Community Health","volume":"15 ","pages":"21501319241242571"},"PeriodicalIF":2.5000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10981848/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Primary Care and Community Health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/21501319241242571","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction/objectives: Colonoscopy completion rates after an abnormal fecal immunochemical test (FIT) are suboptimal, resulting in missed opportunities for early detection and prevention of colorectal cancer. Patient navigation and structured follow-up may improve colonoscopy completion, but implementation of these strategies is not widespread.
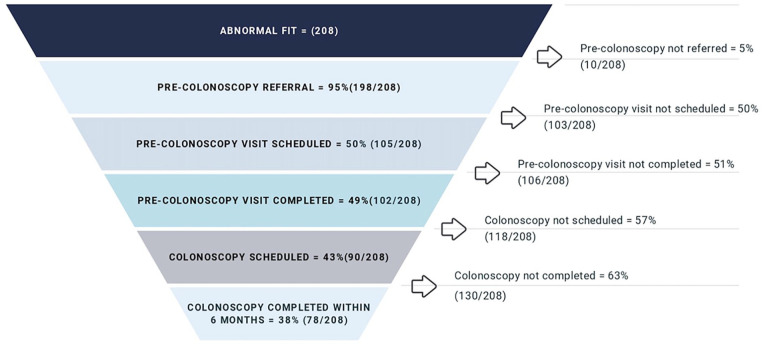
Methods: We conducted a quality improvement study using a Plan-Do-Study-Act (PDSA) Model to increase colonoscopy completion after abnormal FIT in a large federally qualified health center serving a diverse and low-income population. Intervention components included patient navigation, and a checklist to promote completion of key steps required for abnormal FIT follow-up. Primary outcome was proportion of patients achieving colonoscopy completion within 6 months of abnormal FIT, assessed at baseline for 156 patients pre-intervention, and compared to 208 patients during the intervention period from April 2017 to December 2019. Drop offs at each step in the follow-up process were assessed.
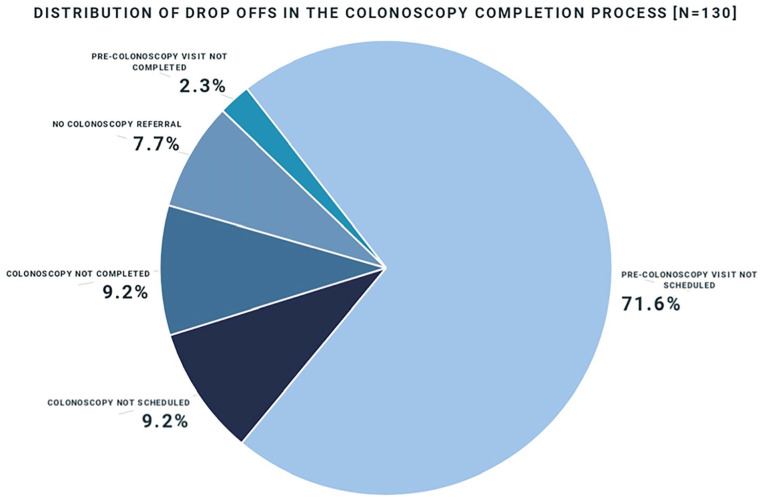
Results: Colonoscopy completion improved from 21% among 156 patients with abnormal FIT pre-intervention, to 38% among 208 patients with abnormal FIT during the intervention (P < .001; absolute increase: 17%, 95% CI: 6.9%-25.2%). Among the 130 non-completers during the intervention period, lack of completion was attributable to absence of colonoscopy referral for 7.7%; inability to schedule a pre-colonoscopy specialist visit for 71.5%; failure to complete a pre-colonoscopy visit for 2.3%; the absence of colonoscopy scheduling for 9.2%; failure to show for a scheduled colonoscopy for 9.2%.
Conclusions: Patient navigation and structured follow-up appear to improve colonoscopy completion after abnormal FIT. Additional strategies are needed to achieve optimal rates of completion.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
